A 46-year-old man with no significant prior medical history or cardiovascular risk factors initially presented with nonexertional chest pain. Electrocardiogram showed no abnormality (Figure 1). Transthoracic echocardiography performed in an outpatient office showed normal biventricular and valvular function but noted a largely homogenous mass in the left atrium measuring 2.3 x 3 cm with no visualized stalk from the interatrial septum (Figure 2). Transesophageal echocardiogram demonstrated 2.6 x 3.3 cm mass in the left atrium protruding into the left upper pulmonary vein (Figure 3). Pre-surgical coronary angiogram revealed normal coronary arteries. Given the location and frequency of left atrial mass, the preoperative diagnosis was left atrial myxoma.
Figure 1: Electrocardiogram on Initial Presentation
Figure 1
Figure 2
Figure 2
Transthoracic echocardiogram shows mildly homogenous mass in the left atrium measuring 3 x 2.3 cm with no visualized stalk from the interatrial septum.
Transthoracic echocardiogram shows mildly homogenous mass in the left atrium measuring 3 x 2.3 cm with no visualized stalk from the interatrial septum.
The patient underwent endoscopic robotic resection of the mass performed with extended endarterectomy of the left pulmonary veins origin and an extensive endothelial-intima resection of the entire left atrium down to the mitral valve leaflets. The extensive resection produced incompetency of the mitral valve that required replacement with a 27 mm bioprosthetic mitral valve. The pathology specimen showed high-grade, undifferentiated sarcoma with spindle and epithelioid morphology (Figure 4), with tumor extension to the inked edges that conferred a positive margin. The patient was started on monthly adjuvant systemic chemotherapy (adriamycin, ifosfamide, and mesna) and completed a total of 6 cycles of adjuvant chemotherapy, with a cumulative doxorubicin 150 mg/m2, ifosfamide 15 g/m2, and mesna 15 g/m2. He also received dexrazoxane 250 mg/m2 for 2 doses to mitigate potential anthracycline cardiotoxicity. Serial imaging surveillance with cardiac magnetic resonance imaging (MRI) and computed tomography of the chest performed every 3 months initially showed no evidence of residual or metastatic disease until cardiac MRI performed 12 months later found small punctate myocardial scar along the mid anterior wall. Another MRI 6 months later revealed new myocardial mass in the mid anterior wall (2.8 x 1.6 cm) with central necrosis (Figure 5), findings consistent with recurrent primary cardiac sarcoma. Cardiothoracic surgeons determined that he was not a candidate for reoperation given the extent and location of the recurrent sarcoma.
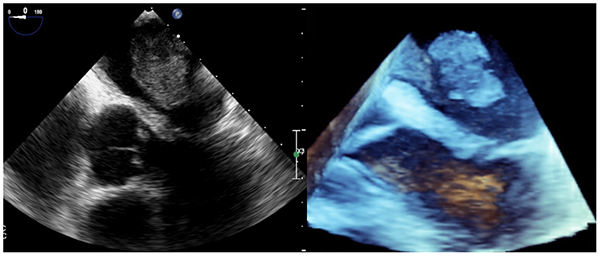
Figure 3
Figure 3
A large 2.6 x 3.3 cm mass in the left atrium protruding into the left upper pulmonary vein shown in five-chamber transesophageal echocardiogram and three-dimensional views.
A large 2.6 x 3.3 cm mass in the left atrium protruding into the left upper pulmonary vein shown in five-chamber transesophageal echocardiogram and three-dimensional views.
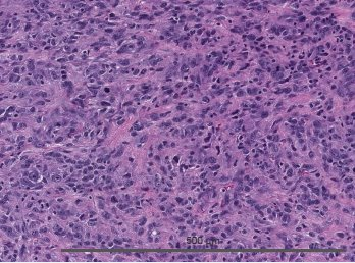
Figure 4
Figure 4
Histologic specimen of high-grade, undifferentiated cardiac sarcoma with spindle and epithelioid morphology.
Histologic specimen of high-grade, undifferentiated cardiac sarcoma with spindle and epithelioid morphology.
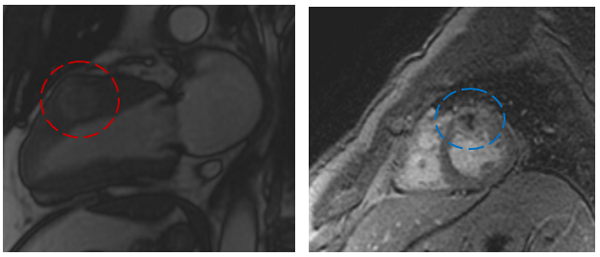
Figure 5
Figure 5
Cardiac MRI shows 3.4 x 1.9 cm mid-anterior left ventricular wall mass in two-chamber view (red circle) and short-axis view (blue circle) with central necrosis (blue circle).
Cardiac MRI shows 3.4 x 1.9 cm mid-anterior left ventricular wall mass in two-chamber view (red circle) and short-axis view (blue circle) with central necrosis (blue circle).
What is the most common malignant cardiac tumor?
Show Answer
The correct answer is: D. Metastatic disease
Metastatic disease to the heart is 40 times more common than primary malignant cardiac tumors.
About 75% of cardiac tumors are benign, and the most common benign cardiac tumor is myxoma. The incidence of malignant cardiac tumor is about 10% of all surgically excised cardiac tumors, and cardiac sarcoma is the most common primary malignant cardiac tumor, accounting for 90% of cases, followed by lymphoma.1 The 2015 World Health Organization classification of cardiac sarcoma includes: angiosarcoma, undifferentiated pleomorphic sarcoma, myxofibrosarcoma, synovial sarcoma, osteosarcoma, leiomyosarcoma, rhabdomyosarcoma, and miscellaneous sarcomas.2 The locations and prognosis of different types of cardiac sarcomas are variables. Angiosarcoma is found most commonly on the right heart chambers and is the most lethal, with rapid recurrence after resection, compared with myxofibrosarcoma, which typically arises from the left heart chambers and has better treatment response. Primary cardiac sarcoma often results in poor prognosis in the younger patient population, with median survival of 6 months and estimated overall survival of only 10% at 9-12 months after diagnosis without surgical resection.3,4 The initial presentations can include congestive heart failure due to intracardiac obstruction, systemic embolization, and atrial and ventricular arrhythmias. This patient presented initially with obstructive symptoms of a large left atrial mass. The optimal management of cardiac sarcoma remains unclear given the overall poor survival and high rates of recurrence after resection. But current literature supports complete surgical resection if possible given the relatively poor response to systemic chemotherapy (median survival 6 months) versus incomplete resection (median survival 11 months) and complete resection (median survival 24 months).5,6 The complete radical resection technique of cardiac autotransplantation involves explantation of the heart to allow for complete ex vivo resection to aim for negative margins, followed by reconstruction, and then reimplantation. In one surgical center's 35 incidences of cardiac autotransplantation in 1998-2013, the survival for primary malignant cardiac sarcoma at 1-year and 2-years was 46% and 28%, respectively.7 Published recommendations include neoadjuvant and adjuvant chemotherapy to improve survival and, in selected cases, radiation therapy.6,8 Patients with recurrent primary cardiac sarcoma are often deemed not operable even with autotransplantation. Most surgical resections are carried out as palliative rather than curative, as in this case. Meticulous imaging surveillance with cardiac MRI and chest computed tomography for ongoing staging and ruling out metastatic disease is of utmost importance. Orthotopic heart transplant and durable ventricular-assist devices can potentially offer a cure or be a bridge to decision for transplant in selected patients with non-metastatic primary cardiac sarcoma, but experience with these approaches is extremely limited, and the reported outcomes are not favorable. There is no other cardiac neoplasm as lethal as primary cardiac sarcoma, and no other cardiac malignancy is as frustrating for the patients, who are often young and in their most productive years, and treating clinicians. Further research and collaboration between multispecialty fields of oncology, cardio-oncology, cardiothoracic surgery, and heart failure transplant are needed to find better therapies for patients with primary cardiac sarcoma.
References
Burke A. Primary malignant cardiac tumors. Semin Diagn Pathol 2008;25:39-46.
Burke A, Tavora F. The 2015 WHO Classification of Tumors of the Heart and Pericardium. J Thorac Oncol 2016;11:441-52.
Leja MJ, Shah DJ, Reardon MJ. Primary Cardiac Tumors. Tex Heart Inst J 2011;38:261-2.
Hamidi M, Moody JS, Weigel TL, Kozak KR. Primary cardiac sarcoma. Ann Thorac Surg 2010;90:176-81.
Putnam JB Jr, Sweeney MS, Colon R, Lanza LA, Frazier OH, Cooley DA. Primary cardiac sarcomas. Ann Thorac Surg 1991;51:906-10.
Blackmon SH, Rice DC, Correa AM, et al. Management of primary pulmonary artery sarcomas. Ann Thorac Surg 2009;87:977-84.
Ramlawi B, Al-Jabbari O, Blau LN, et al. Autotransplantation for the resection of complex left heart tumors. Ann Thorac Surg 2014;98:863-8.
Ostrowski S, Marcinkiewicz A, Kośmider A, Jaszewski R. Sarcomas of the heart as a difficult interdisciplinary problem. Arch Med Sci 2014;10:135-48.