An 86-year-old man with a history of coronary artery disease, hypertension, and hyperlipidemia presented with chest pain and acute dyspnea. His home medications included aspirin and valsartan.
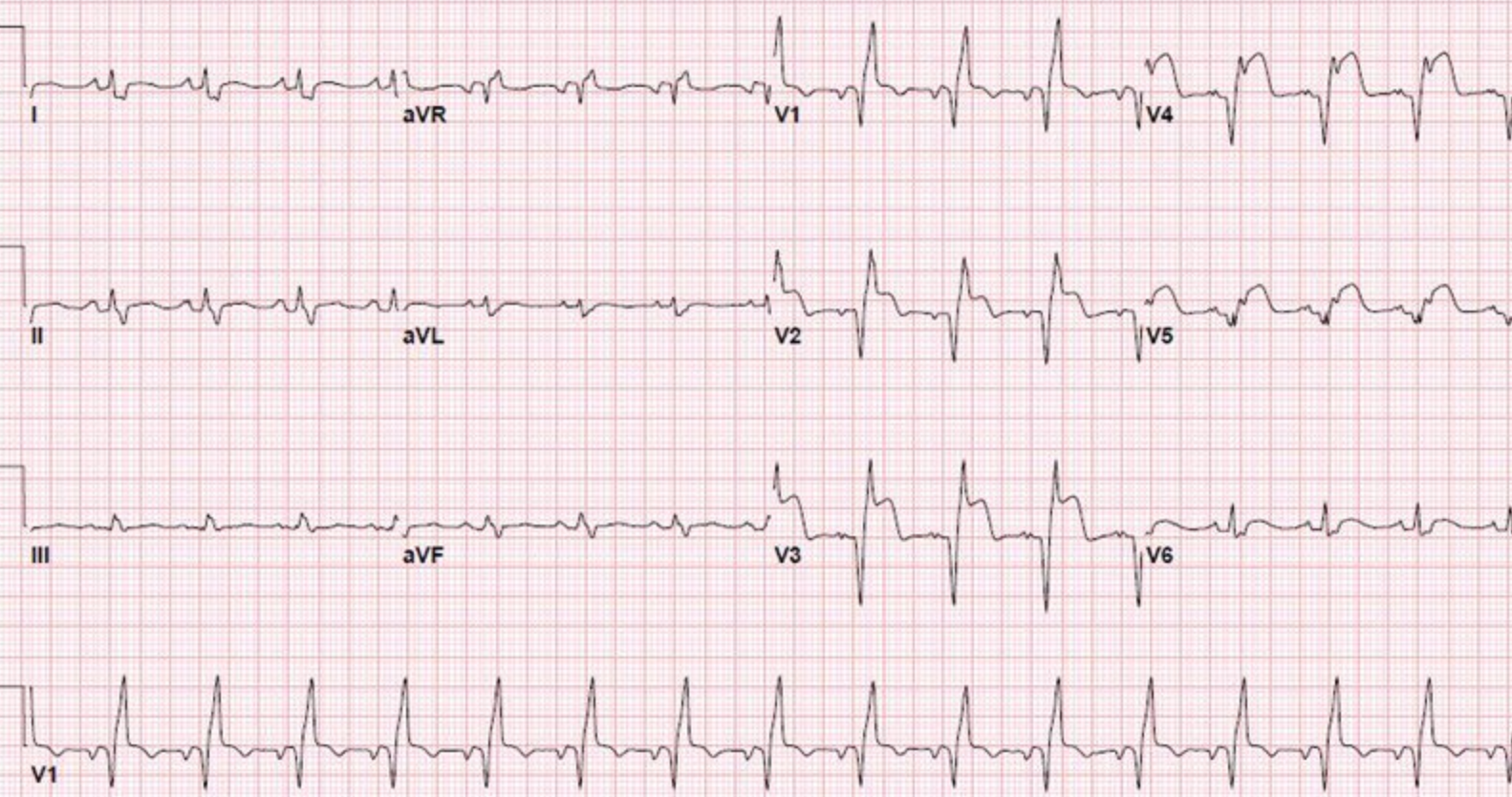
His initial examination was notable for hypoxia on room air (89%) that improved with 2 liters oxygen supplementation. His blood pressure was 95/78 mmHg, and his heart rate was regular at 92 beats per minute. The chest had bilateral inspiratory crackles, and there was 1+ peripheral edema. The electrocardiogram showed normal sinus rhythm with a right bundle branch block and anterior ST-segment elevation (Figure 1). Chest radiograph showed pulmonary vascular congestion, edema, and cardiac enlargement. The troponin I was 10.0 ng/mL (normal is 0.00-0.50 ng/mL), platelet was 160 K/mm3 (normal is 150-450), creatinine was 4.0 mg/dL, and pro-NT brain natriuretic peptide was 2,649 pg/mL (normal is ≤125 pg/mL). The patient was thought to be in cardiogenic shock. The patient underwent emergent cardiac catheterization. Coronary angiography revealed a 95% calcified lesion in the ostial, proximal, and mid-left anterior descending artery with Thrombolysis in Myocardial Infarction 2 flow and a 30% lesion in the ostial left main coronary (Videos 1-2). The left ventricular ejection fraction was ~20%, and end-diastolic pressure 15 mmHg. An intra-aortic balloon pump was placed, and cardiothoracic surgery was consulted due to the high-risk anatomy. The patient was declined for emergent coronary artery bypass grafting by cardiothoracic surgery, and percutaneous coronary intervention (PCI) was recommended.
Figure 1
Figure 1
Video 1
Video 2
Prior to attempting PCI on this patient, which of the following next steps would provide the most rapid inhibition of platelets and would also not be influenced by concomitant renal insufficiency?
Show Answer
The correct answer is: D. Treatment with cangrelor
This case presents an 86-year-old man with an ST-segment elevation myocardial infarction, renal insufficiency, pulmonary edema, cardiogenic shock, and complex coronary artery disease who was deemed not a surgical candidate. Early revascularization is indicated due to cardiogenic shock and ongoing ischemic symptoms. The patient's sole antiplatelet effect is due to aspirin at the time of catheterization. Oral P2Y12 inhibitor therapy is indicated, but the maximal pharmacodynamic effect will not be reached by the time of the intervention.1 Moreover, a delayed pharmacodynamic effect of oral antiplatelet therapy has been reported in shock.2 Both the parenteral agents noted (eptifibatide and cangrelor) would provide immediate and potent platelet inhibition, but eptifibatide clearance is affected by renal function and cangrelor clearance is not.3
Cangrelor is an adenosine triphosphate analog that selectively and specifically blocks P2Y12 receptor-mediated platelet activation in a direct, reversible, and competitive fashion. It is the only intravenous P2Y12 inhibitor available for clinical use with a rapid onset occurring within minutes and a plasma half-life of 3-6 minutes with rapid platelet function recovery within 30-60 minutes after discontinuation of infusion.4
Cangrelor was approved for clinical use by the US Food and Drug Administration as an adjunct to PCI to reduce the risk of myocardial infarction, repeat coronary revascularization, and stent thrombosis in patients not adequately pretreated with a P2Y12 platelet inhibitor and not being given a glycoprotein IIb/IIIa inhibitor.5 Cangrelor was extensively studied in the CHAMPION PCI (Cangrelor Versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition–PCI), CHAMPION PLATFORM (Clopidogrel Versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition–PLATFORM), and CHAMPION PHOENIX (Cangrelor vs. Standard Therapy to Achieve Optimal Management of Platelet Inhibition) trials for use in patients undergoing PCI with stable angina or acute coronary syndrome with obstructive coronary artery disease.6-8 In this patient, due to the potential benefit of rapid P2Y12 inhibition in the setting of renal insufficiency, cangrelor therapy is the correct choice.
References
Gurbel PA, Bliden KP, Butler K, et al. Randomized double-blind assessment of the ONSET and OFFSET of the antiplatelet effects of ticagrelor versus clopidogrel in patients with stable coronary artery disease: the ONSET/OFFSET study. Circulation 2009;120:2577-85.
Orban M, Mayer K, Morath T, et al. The impact of therapeutic hypothermia on on-treatment platelet reactivity and clinical outcome in cardiogenic shock patients undergoing primary PCI for acute myocardial infarction: Results from the ISAR-SHOCK registry. Thromb Res 2015;136:87-93.