A 73-year-old male with history of atrial fibrillation, coronary disease s/p CABG x4, ischemic cardiomyopathy (EF 40-45%) and end-stage renal disease on hemodialysis presents for evaluation of persistent volume overload. Patient has noted fluid retention, dyspnea on exertion and orthopnea despite four dialysis sessions per week. Blood pressure is 107/56, heart rate is 103 and SpO2 is 98% on room air. Physical exam is notable for irregularly irregular rhythm, 3/6 systolic murmur increased with inspiration, JVD 25cm (1-day post dialysis), ascites and 2+ peripheral edema.
Transthoracic echocardiogram shows LV ejection fraction 43%, dilated RV with moderately decreased RV function, abnormal septal bounce, severe biatrial dilation, severe mitral regurgitation and severe tricuspid regurgitation and possible tethering of RA, LA and lateral wall of LV with thickened pericardium.
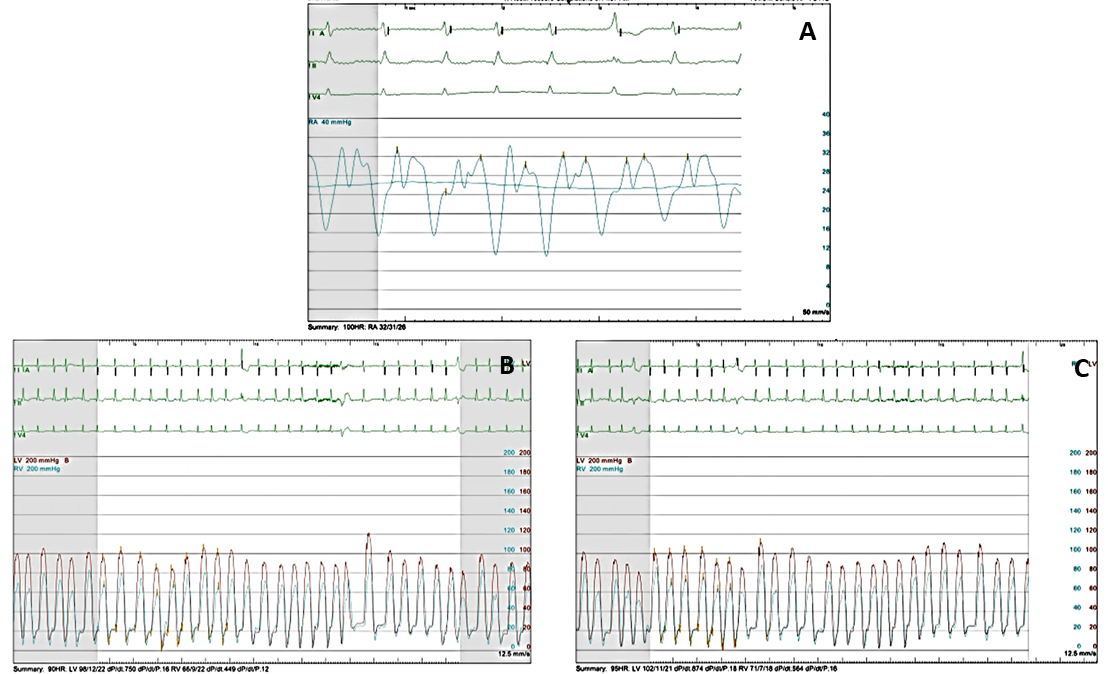
Hemodynamic tracings from the patient are shown below. Figure 1A shows RA tracing while Figures 1B and 1C show simultaneous RV and LV tracings.
Figure 1
Which of the following is the most likely etiology of his findings?
Show Answer
The correct answer is: C. Severe tricuspid regurgitation.
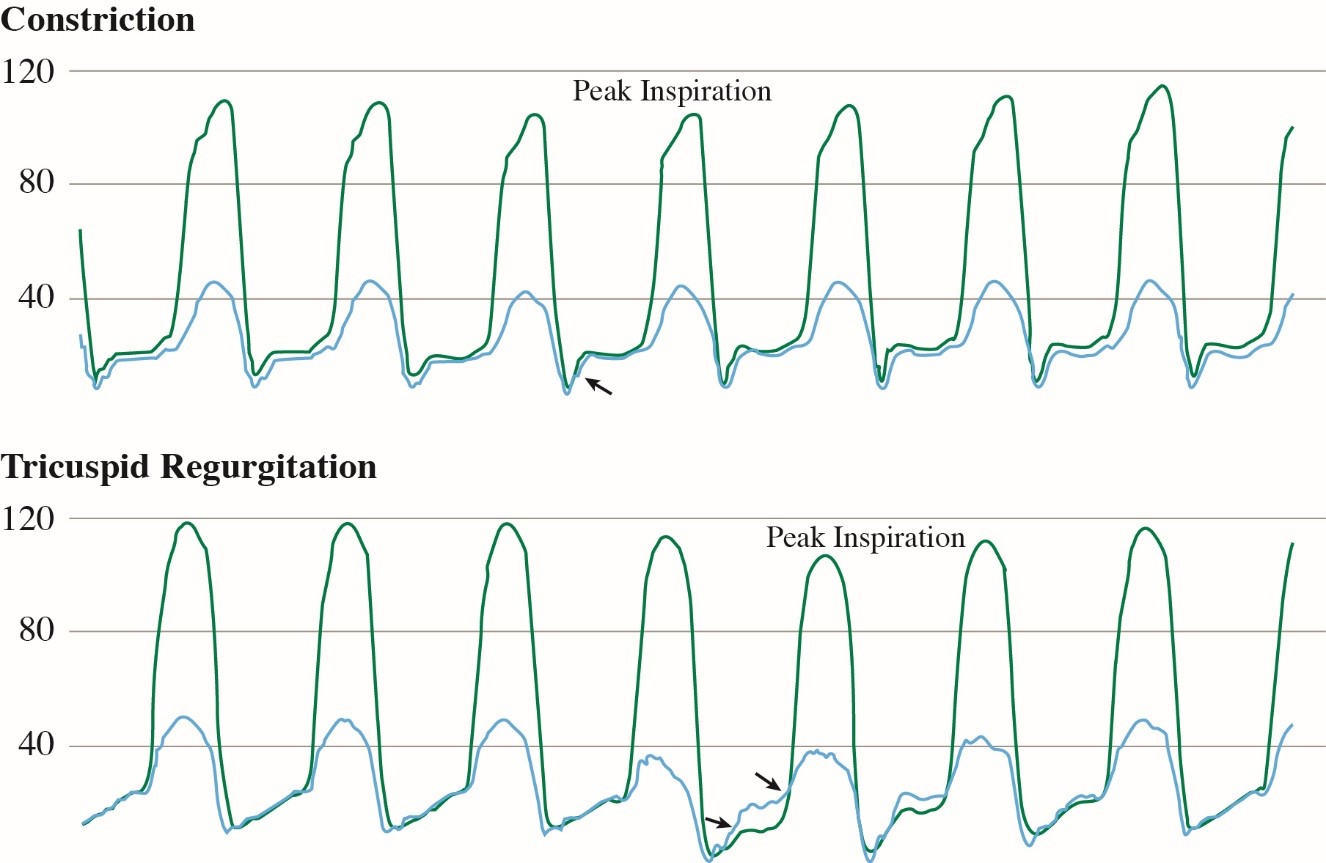
The patient has many findings consistent with constriction on his tracings, including elevated RA pressure, prominent y descent, square root sign, equalization of LV/RV diastolic pressure and ventricular interdependence. An important distinction between constriction and tricuspid regurgitation is seen on deep inspiration. While in constriction diastolic pressures between the LV and RV remain equal throughout inspiration and expiration, in severe TR, during deep inspiration there is a higher RV diastolic pressure with deeper and steeper RV filling wave and a drop in LV diastolic pressure (see image below, adapted from Jaber et al.). This pattern is also seen in our patient.
Figure 2
As noted above, constriction and severe tricuspid regurgitation share many common findings on hemodynamic tracings. In constriction, cardiac chambers are all confined within a rigid pericardium. In severe TR, the dilated RV can constrict the LV and can cause a similar pattern. However, in constriction, the flow to the RV is limited by the pericardium and thus there is very little increase in flow through the RV in inspiration. In contrast, in severe TR, there is no limitation of low into the RV leading to an increase in RV diastolic filling in inspiration. Furthermore, in constriction, you generally see ventricular interdependence with inspiration, which you do not see in the patient's waveforms. In restrictive cardiomyopathy, there is generally blunted x-descent of the atrial waveform, which is not present in this case, making restrictive cardiomyopathy less likely. There are a-waves on the right atrial waveform, making atrial fibrillation incorrect.
Our patient underwent cardiac surgery with mitral valve replacement, tricuspid valve repair, and pericardectomy. The pericardium was only mildly thickened on visual inspection and pathology confirmed that the pericardium was normal.
References
Jaber WA, Sorajja P, Borlaug BA, Nishimura RA. Differentiation of tricuspid regurgitation from constrictive pericarditis: novel criteria for diagnosis in the cardiac catheterisation laboratory. Heart 2009;95:1449-54.
Geske JB, Anavekar NS, Nishimura RA, Oh JK, Gersh BJ. Differentiation of constriction and restriction: complex cardiovascular hemodynamics. J Am Coll Cardiol 2016;68:2329-47.
Talreja DR, Nishimura RA, Oh JK, Holmes DR. Constrictive pericarditis in the modern era: novel criteria for diagnosis in the cardiac catheterization laboratory. J Am Coll Cardiol 2008;51:315-9.