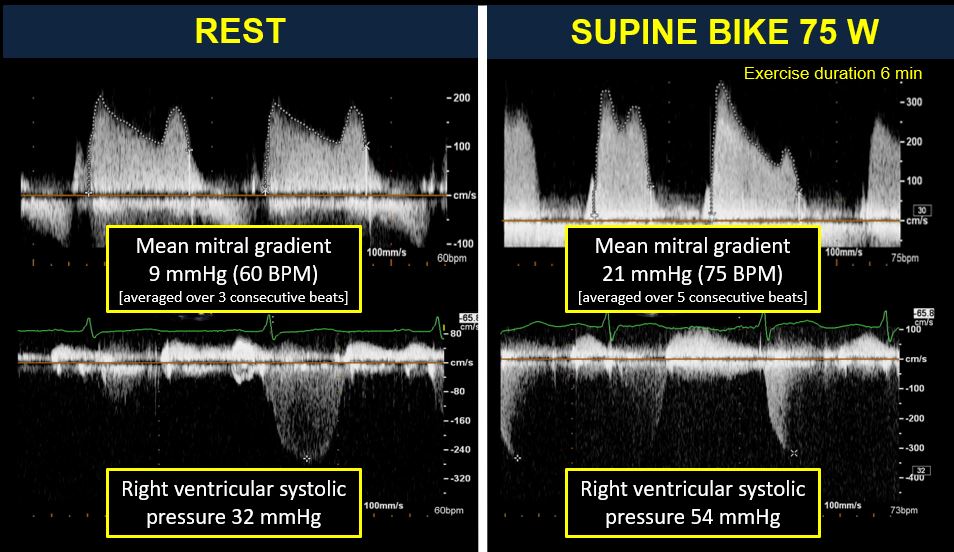
A 75-year-old female patient with history of hypertension and diabetes presented 3 years previously with worsening fatigue and exercise intolerance. Evaluation at that time revealed the presence of severe aortic stenosis, severe mitral annular calcification (MAC), and three-vessel coronary artery disease. She subsequently underwent an aortic valve replacement and multivessel coronary artery bypass grafting. Intraoperatively, inspection of the mitral valve showed an extensive circumferential calcification of the valve that was densely embedded across the mitral annulus. Because decalcification maneuvers would be very challenging technically and associated with increased risk of atrioventricular groove disruption, no intervention was performed on the mitral valve. The patient did well following the operation but re-presented 3.5 years later with recurrent progressive fatigue and exertional dyspnea. She can walk for only 1 block before having to stop due to dyspnea. She reported 10 kg of weight gain in the preceding year from inactivity. Repeat evaluation showed the presence of a normally functioning aortic prosthesis, preserved biventricular systolic function, and patent coronary grafts. Severe MAC was again noted (Figure 1). Averaged mean mitral diastolic gradient was 9 mmHg at rest (heart rate was 60 BPM); this is associated with mild mitral regurgitation (MR). As part of her evaluation, a supine bike stress echocardiogram was performed; the results are summarized in Figure 2.
Figure 1
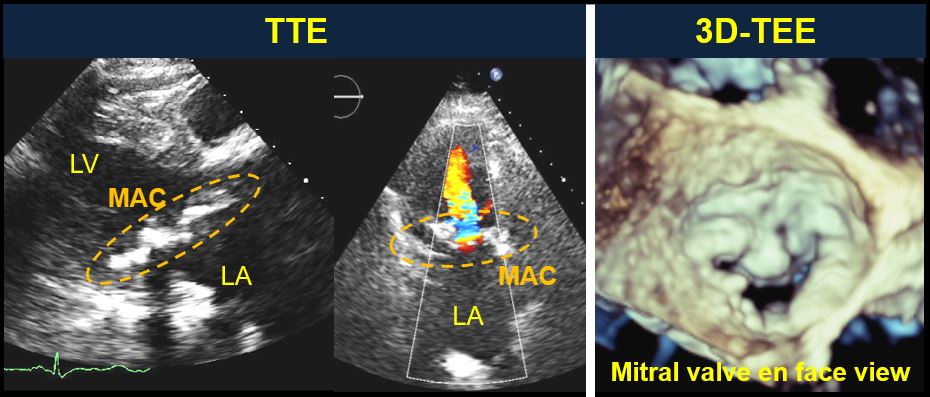 TTE, transthoracic echocardiography; 3D TEE, three-dimensional transesophageal echocardiography; LA, left atrium; LV, left ventricle
TTE, transthoracic echocardiography; 3D TEE, three-dimensional transesophageal echocardiography; LA, left atrium; LV, left ventricle
Figure 2
The correct answer is: C. Supine bike stress echocardiogram is recommended for the assessment of MS; however, when a patient is unable to exercise, dobutamine stress echocardiogram is a reasonable alternative.
For patients who are unable to exercise, dobutamine stress echocardiogram can be used as an alternative test to assess MS severity. Assessment of MS severity in the context of severe MAC is challenging and is best performed using mitral valve area calculation by continuity equation, although its use may be limited in the presence of concomitant aortic and mitral valve regurgitation.1 Alternatively, whenever feasible, 3D-TEE planimetry of mitral valve area can also be used to grade hemodynamic severity produced by the severe MAC. Although mitral valve gradient estimation from the continuous wave Doppler is helpful to give an indicator of MS severity, it is highly dependently on other factors such as heart rate, cardiac output, and associated MR. Thus, in isolation, transmitral gradient has not been included in the criteria for MS severity assessment within the current guidelines.2 Meanwhile, mitral valve area by pressure half time is highly influenced by LA and LV compliance, delayed ventricular relaxation, and concomitant aortic regurgitation. Therefore, it has limited utility in estimating mitral valve area in elderly patients with calcific MS in whom diastolic dysfunction is highly prevalent. Therefore, answer A is incorrect.
Based on MESA (Multi-Ethnic Study of Atherosclerosis), which included 6,814 patients, the overall prevalence of MAC was 9%.3 Elevated mean transmitral gradient is found quite rarely among patients with MAC, occurring in 0.2% of patients with prevalence increasing to 2.5% in patients >90 years of age.1 Meanwhile, in a study that reviewed 24,380 echocardiograms, MAC was present in 11.7% of patients with MR versus 4.3% without MR.4 These data suggest that MAC is more commonly associated with MR rather than stenosis. Therefore, answer B is incorrect.
Exercise stress echocardiography is the preferred modality for assessment of hemodynamic consequences of MS because it allows evaluation of mean mitral gradient and systolic pulmonary artery pressure with exercise. Typically, an average value from 3 consecutive beats is reported in sinus rhythm and at least 5 beats in those with irregular heart rate or variable RR interval. In patients who are unable to exercise, dobutamine stress echocardiogram can be used to assess mitral valve gradient during stress, although it is not recommended for assessment of systolic pulmonary artery pressure.5 Therefore, answer C is correct. MS is diagnosed as severe if the mean gradient is >15 mmHg with exercise or >18 mmHg during dobutamine infusion.5
Percutaneous balloon mitral valvuloplasty works by disrupting commissural fusion and thus plays an important role in patients with rheumatic MS. It is, however, not an option in patients with MAC because calcification in MAC involves the annulus and base of the leaflets without commissural fusion.2 Therefore answer D is incorrect.
Transcatheter mitral valve replacement-in-MAC procedure, using a balloon expandable valve, is a feasible treatment option in extreme surgical risk patients with severe MAC. Based on recent registry data, however, the procedure is associated with high 30-day and 1-year all-cause mortality (25% and 53.7%, respectively).6 But in those who survived beyond 30 days post-procedure, up to 64% of patients were alive at 1 year and have sustained improvements of symptoms and functional class. Therefore, answer E is incorrect because 1-year all-cause mortality was in fact much greater than 25%.
References
- Eleid MF, Foley TA, Said SM, Pislaru SV, Rihal CS. Severe Mitral Annular Calcification: Multimodality Imaging for Therapeutic Strategies and Interventions. JACC Cardiovasc Imaging 2016;9:1318-37.
- Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:2438-88.
- Kanjanauthai S, Nasir K, Katz R, et al. Relationships of mitral annular calcification to cardiovascular risk factors: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2010;213:558-62.
- Movahed MR, Saito Y, Ahmadi-Kashani M, Ebrahimi R. Mitral annulus calcification is associated with valvular and cardiac structural abnormalities. Cardiovasc Ultrasound 2007;5:14.
- Lancellotti P, Pellikka PA, Budts W, et al. The Clinical Use of Stress Echocardiography in Non-Ischaemic Heart Disease: Recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr 2017;30:101-38.
- Guerrero M, Urena M, Himbert D, et al. 1-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol 2018;71:1841-53.