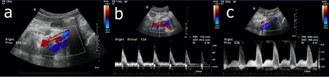
A 35-year-old male plumber with type 1 diabetes presents with right lower extremity and buttock claudication. He previously had undergone recanalization of an occlusion of the right external iliac artery one year prior at another institution. Duplex ultrasonography showed >75% stenosis (Figure 1a) in the right external iliac artery with a 6-fold increase in the peak systolic velocity from the distal right common iliac to proximal external iliac artery (Figure 1b and 1c). Records of the previous intervention were obtained and notable for a residual 21 mm Hg translesional systolic gradient despite aggressive balloon dilatation pre and post stent placement. He was offered a supervised exercise program but was unable to attend given full time employment. Given the imaging findings, known residual gradient and ongoing lifestyle-limiting claudication refractory to conservative measures, he was referred for invasive angiography.
Figure 1
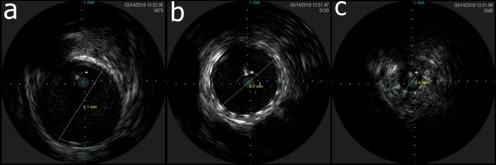
Angiography performed via six French contralateral access showed fluoroscopically evident stent under-expansion correlating with a severe stenosis (Figure 2a and 2b). Despite aggressive angioplasty with a 5mm balloon at up to 24 atmospheres, significant recoil was seen. Intravascular ultrasound was performed and showed the stenosis of interest to be fibrotic material externally compressing the stent with a lack of atherosclerosis in the remainder of the vessel (Figure 3a-c).
Figure 2
Figure 3
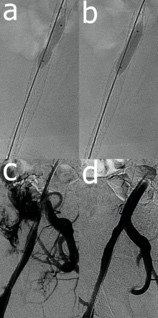
After upsizing to 7F crossover access, balloons up to 8mm in diameter were used for high pressure angioplasty with similar results to the initial angioplasty. A 6x20mm cutting balloon was then deployed at 20 atm with sudden expansion of the balloon (Figure 4a and 4b). Following this, the patient became hypotensive, nauseous and diaphoretic. Angiography revealed a right external iliac artery perforation (Fig 4c). Balloon tamponade was performed with an 8x20mm balloon. Ipsilateral 7F access was obtained and a guidewire advanced retrograde to the aorta. An 8x38 iCAST™ stent was deployed via this access followed by further balloon tamponade with a 9mm balloon. Final angiography showed no residual extravasation (Figure 4d), and the patient's hemodynamics had returned to baseline.
Figure 4
The correct answer is: C. Endofibrosis
The intravascular ultrasound (IVUS) images showed fibrotic tissue external to the stent with compression of the stent by the tissue. This is consistent with previous histologic examinations of endofibrosis showing intimal fibrosis without atherosclerosis or inflammation.1 Though this is typically seen in athletes,1,2 this patient had a job that led to significant squatting similar to that seen in bicyclists. Additionally, lesions have been seen in the entire iliofemoral system.3 Though there is no clear etiology, proposed mechanisms include arterial kinking, tethering of the iliac artery by the psoas arterial branch and fibrous tissue, muscular hypertrophy, and mechanical stress and hemodynamic injury leading to arterial remodeling with intimal thickening on histology.2-4,5-9 Though treatment of endofibrosis has classically been surgical, there have been recent reports of percutaneous treatment of this disease.4,10
This does not represent stent fracture as there was no evidence of strut fracture on IVUS or fluoroscopy even after aggressive dilatation. In-stent restenosis would have been seen as neoinitimal hyperplasia within the stent on IVUS and the stent would have appeared relatively well expanded. There was no calcification noted on angiography or IVUS that would have led to stent under-expansion.
References
- Abraham P, Saumet JL, Chevalier JM. External iliac artery endofibrosis in athletes. Sports Med 1997;24:221-26.
- Peach G, Schep G, Palfreeman R, Beard JD, Thompson MM, Hinchliffe RJ. Endofibrosis and kinking of the iliac arteries in athletes: a systematic review. Eur J Vasc Endovasc Surg 2012;43:208-17.
- Scavee V, Stainier L, Deltombe T, et al. External iliac artery endofibrosis: a new possible predisposing factor. J Vasc Surg 2003;38:180-182.
- Rousselet MC, Saint-Andre JP, L'Hoste P, Enon B, Megret A, Chevalier JM. Stenotic intimal thickening of the external iliac artery in competition cyclists. Hum Pathol 1990;21:524-29.
- Collaborators I. Diagnosis and management of iliac artery endofibrosis: results of a delphi consensus study. Eur J Vasc Endovasc Surg 2016;52:90-8.
- Lim CS, Gohel MS, Shepherd AC, Davies AH. Iliac artery compression in cyclists: mechanisms, diagnosis and treatment. Eur J Vasc Endovasc Surg 2009;38:180-86.
- Bender MH, Schep G, de Vries WR, Hoogeveen AR, Wijn PF. Sports-related flow limitations in the iliac arteries in endurance athletes: aetiology, diagnosis, treatment and future developments. Sports Med 2004;34:427-42.
- D'Abate F, Paraskevas KI, Oates C, Palfreeman R, Hinchliffe RJ. Color doppler ultrasound imaging in the assessment of iliac endofibrosis. Angiology 2017;68:225-32.
- Feugier P, Chevalier JM. Endofibrosis of the iliac arteries: an underestimated problem. Acta Chir Belg 2004;104:635-40.
- Maree AO, Ashequl Islam M, Snuderl M, et al. External iliac artery endofibrosis in an amateur runner: hemodynamic, angiographic, histopathological evaluation and percutaneous revascularization. Vasc Med 2007;12:203-06.