A 50 year-old male with history of recently diagnosed Graves' disease, multiple sclerosis and benign prostatic hyperplasia presented to the hospital with chest pain concerning for unstable angina. Initial work-up for his cardiac chest pain, including a coronary angiogram and an echocardiogram showed non-obstructive coronary artery disease, and a severely stenotic bicuspid aortic valve. He subsequently underwent aortic root enlargement with a bovine pericardial patch and bioprosthetic aortic valve replacement without complication. Twenty-three days later, however, he presented to the emergency department endorsing right-sided pleuritic-type chest pain and low-grade fevers.
His medications on presentation included: methimazole, metoprolol tartrate, furosemide, aspirin, atorvastatin, warfarin, dimethyl fumarate and tamsulosin. His vitals signs on presentation were significant for tachycardia (120 bpm) and low-grade fever (100.9 F / 38.2 C) with a low normal resting blood pressure of 98/63 mmHg.
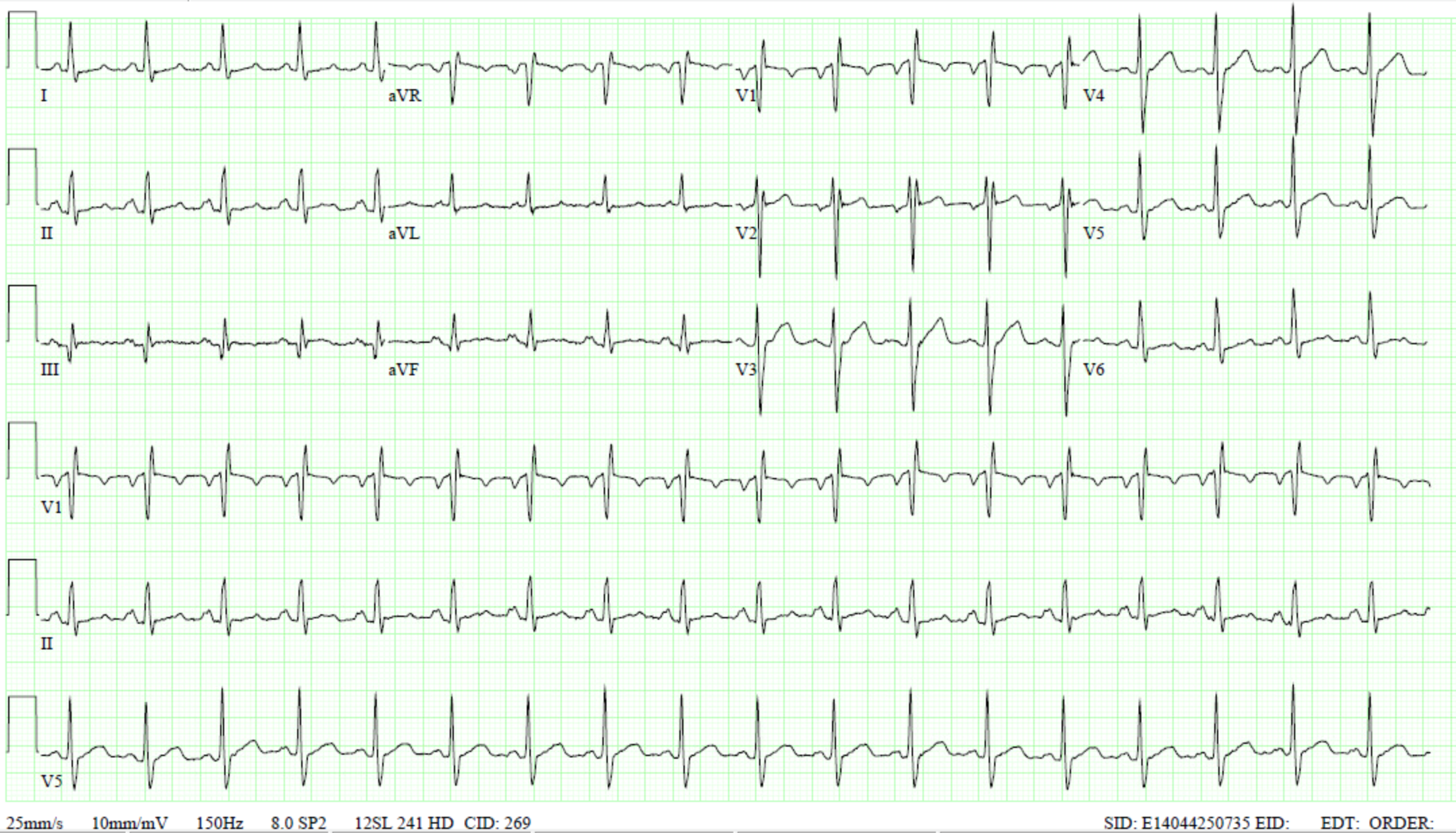
His initial ECG showed sinus tachycardia with incomplete right bundle branch block and possible left atrial enlargement:
ECG
Initial laboratory work-up showed normal troponin (<0.01ng/mL), slightly elevated B-natriuretic peptide of 122pg/mL (0-100pg/mL), normal white blood cell count 7.56k/uL (3.73-10.1k/uL), slight anemia with a hemoglobin of 10.1g/dL (13.4 – 16.8 g/dL), normal platelet count of 337k/uL (146 – 337k/uL), low thyroid stimulating hormone < 0.008uIU/mL (0.55 – 4.78uIU/mL), and normal Free T4 1.06ng/dL (0.89 – 1.76ng/dL).
Initial concern in the post-operative setting was pulmonary embolism, for which a computed tomography (CT) chest was ordered. This showed no signs of pulmonary embolism, but revealed bilateral pleural effusions with atelectasis (Figure 1). Transthoracic echocardiogram (TTE) revealed a normal left ventricle ejection fraction (LVEF) of 60% with trivial pericardial effusion and no valve vegetations.
With overall reassuring tests and labs, he was discharged home, yet presented again 14 days later complaining of persistent symptoms. A repeat CT chest was performed and showed interval worsening moderate-sized right and small left pleural effusions, which were now partially loculated. A therapeutic thoracentesis was performed and yielded 165mL of pleural fluid. Pleural fluid analysis showed:
LDH 737U/L (serum 183U/L), glucose 110mg/dL (serum 127mg/dL), triglycerides 51, protein 4.1g/dL (serum 7.1g/dL), suggesting an exudative effusion based on Light's criteria, with fluid protein more than 0.5 of serum protein and lactate dehydrogenase (LDH) more than 0.6 or more than two-thirds of serum levels. Bacterial and fungal cultures were also negative.
Due to concerns for pericarditis, he was discharged on ASA 325mg daily, colchicine 0.6mg once daily, and 400mg ibuprofen as needed. He returns to the hospital 25 days later with diffuse body aches, dyspnea, fevers, chills and now left sided pleuritic chest pain. Repeat chest imaging shows again worsening bilateral effusions. A repeat TTE was ordered to assess for pericarditis with possibly worsening pericardial effusion. The echocardiogram showed stable systolic LV function (LVEF of 65%) and normal appearing pericardium without signs of underlying constrictive pericarditis. Of note, the inflammatory markers were elevated despite the anti-inflammatory regimen prescribed (ESR 62mm/h, CRP 5.2mg/dL).
Due to his persistent symptoms, now more than 60 days after surgery, with elevated inflammatory markers and no major changes on transthoracic echo, a cardiac magnetic resonance imaging (MRI) is ordered for further clarification.
Figure 1
What is the most likely cause of his clinical picture?
Show Answer
The correct answer is: E. Post-pericardiotomy syndrome
This patient's clinical picture is consistent with post-pericardiotomy syndrome (PPS), a form of post cardiac injury syndrome (PCIS). PCIS is a broad definition that encompasses:
Post-pericardiotomy syndrome: pericarditis after undergoing pericardiotomy during cardiothoracic surgery, which is most commonly seen after aortic and mitral valve replacement compared to coronary artery bypass graft surgery1
Post myocardial infarction pericarditis (Dressler's Syndrome): triggered by myocardial necrosis2,3
Post-traumatic pericarditis: secondary to either iatrogenic (e.g.: percutaneous coronary intervention (PCI) or accidental injury
Post-pericardiotomy syndrome (PPS) is found to occur in 10-40% of patients undergoing cardiac surgery. Uncomplicated post-operative pleural effusions can happen as a consequence of the surgical procedure itself, usually 1-2 days after surgery, and are usually not progressive. Simple post-operative effusions are also not commonly associated with respiratory symptoms and lack signs of systemic inflammation.2-4
PCIS is believed to have an underlying autoimmune pathogenesis, triggered by pericardial and/or pleural tissue damage caused by myocardial necrosis (Dressler's syndrome), accidental thoracic trauma, iatrogenic trauma (e.g. during PCI) or surgical trauma, as depicted by our patient's case, who presented 25 days after a bovine pericardial patch aortic root enlargement.
Patients with PCIS mostly present with chest pain (>80%), low-grade fevers (50-60%) and dyspnea (50-60%). Laboratory findings of systemic inflammation (Leukocytosis and elevated C-reactive protein (CRP) also help support diagnosis. Typical pericarditis ECG pattern can also occur (widespread ST elevations and PR depressions).3
The European Society of Cardiology (ESC) in the 2015 Pericardial disease guidelines2 proposed the diagnostic criteria for PCIS, requiring prior injury of pericardium and/of myocardium and at least two of the following:
Fever without alternative causes
Pleuritic or pericarditic chest pain
Pleural or pericardial friction rub
Evidence of pericardial effusion
Pleural effusion with elevated CRP
It is often difficult to differentiate PPS from simple mechanical consequences of cardiac surgery. Although our patient did not present with significant pericardial effusion after two repeated echocardiograms within one month, his pleural effusions and elevated CRP with pleuritic chest pain support the diagnosis of PCIS. Cardiac MRI further confirmed the diagnosis by demonstrating both pericardial and pleural inflammation in the presence of an elevated CRP and low-grade fevers.
Although cardiac MRI is not routinely recommended in post-cardiac injury syndrome, its role in acute and constrictive pericarditis is rapidly evolving. Using a series of sequences including dark-blood axial, bright-blood axial slices and steady state free precession (SSFP) cine sequence, we can readily identify a thickened pericardium, pericardial effusions and pleural effusions. Cardiac MRI clearly sets itself apart from the other imaging modalities (echocardiography and cardiac CT) for its ability to characterize the pericardium. In the presence of an increased signal on T2 short tau inversion recovery (T2-STIR) images, an edematous pericardium can be identified. Moreover, 15 minutes following injection of a gadolinium based enhancing agent, pericardial delayed enhancement can be appreciated, signifying pericardial inflammation. In the presence of increased pericardial signal on T2-STIR and DHE sequences, acute inflammation is diagnosed. Once the edema resolved (normal pericardial T2-STIR signal) a subacute phase of inflammation is diagnosed, which can be appreciated in the above case. Subsequent resolution of both T2STIR and DHE suggests a healed pericardium.5
Figure 1
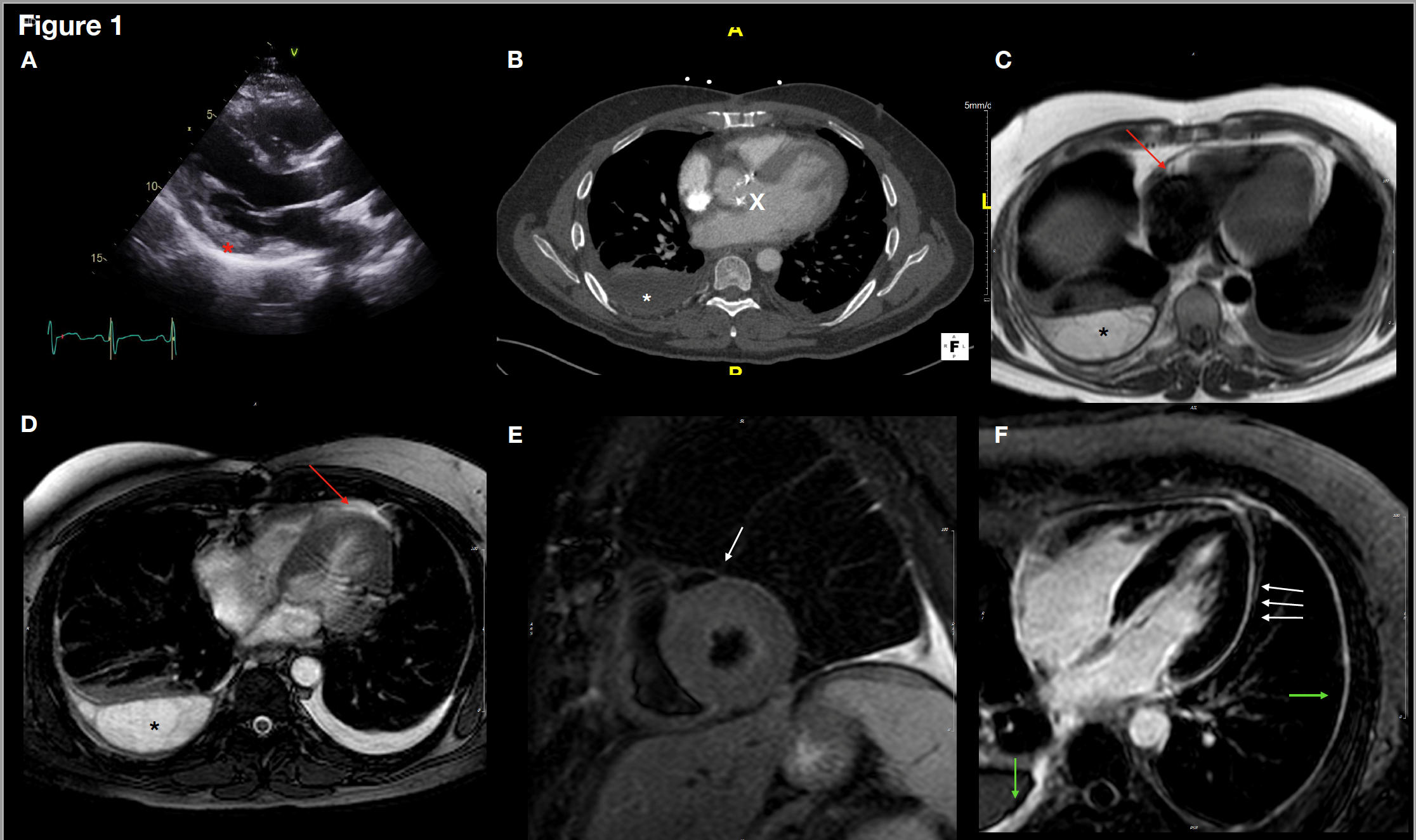
(A) Parasternal long axis view on transthoracic echocardiogram demonstrating a thickened pericardium. (B) Axial CT chest demonstrating small right and tiny left pleural effusions and the previous AVR (X). (C) Cardiac MRI Axial black blood image demonstrating bilateral pleural effusions and a thickened pericardium (Red arrow). (D) Cardiac MRI Axial bright blood image demonstrating bilateral pleural effusions and a small pericardial effusion (Red arrow). (E) T2 Short Tau inversion recovery showing no pericardial enhancement (white arrow). (F) Delayed hyperenhancement sequences on CMR demonstrating circumferential pericardial delayed enhancement as well as enhancement of the right and left pleura. This constellation of findings is consistent with a subacute stage of pericardial and pleural inflammation in the setting of post cardiac injury syndrome.
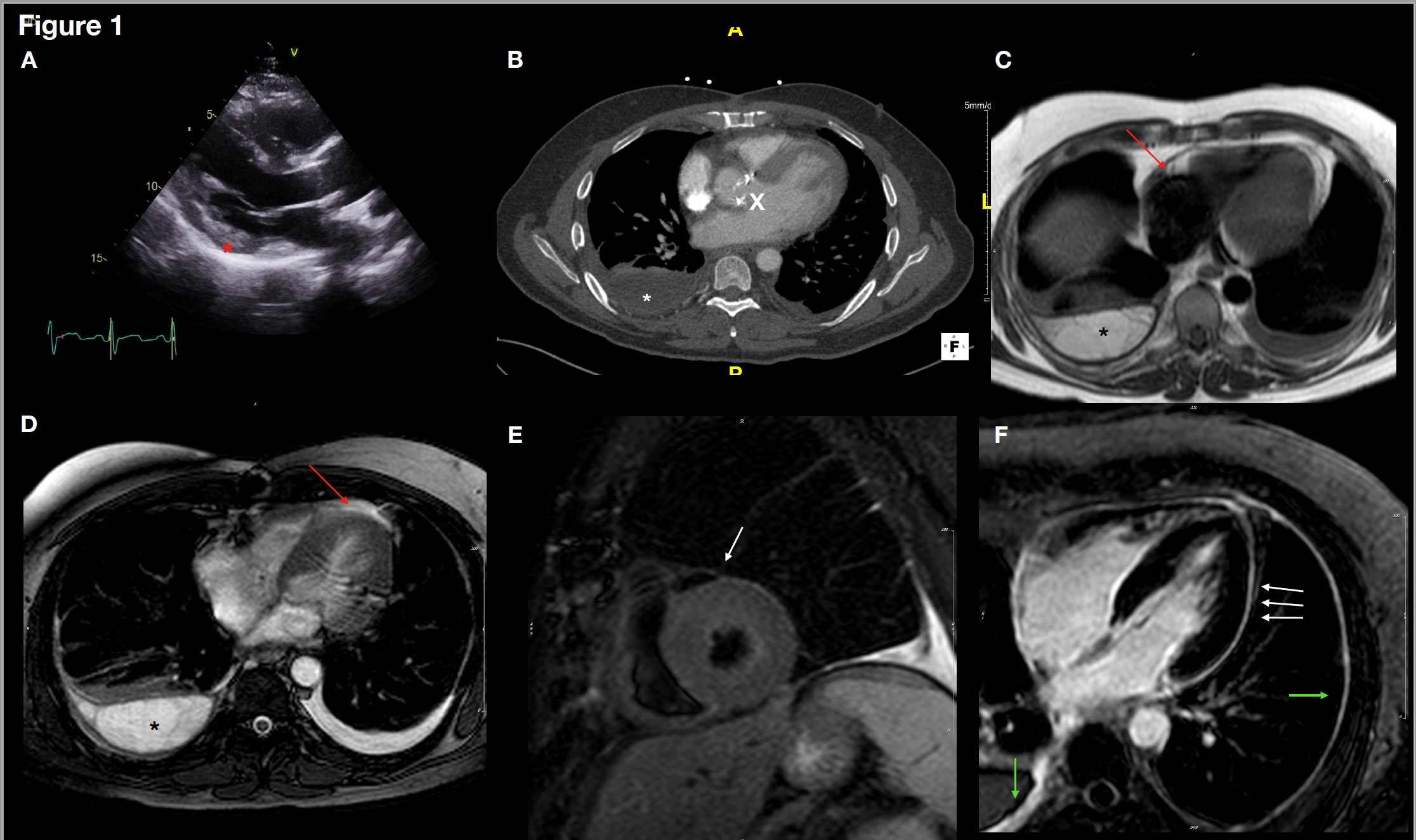
(A) Parasternal long axis view on transthoracic echocardiogram demonstrating a thickened pericardium. (B) Axial CT chest demonstrating small right and tiny left pleural effusions and the previous AVR (X). (C) Cardiac MRI Axial black blood image demonstrating bilateral pleural effusions and a thickened pericardium (Red arrow). (D) Cardiac MRI Axial bright blood image demonstrating bilateral pleural effusions and a small pericardial effusion (Red arrow). (E) T2 Short Tau inversion recovery showing no pericardial enhancement (white arrow). (F) Delayed hyperenhancement sequences on CMR demonstrating circumferential pericardial delayed enhancement as well as enhancement of the right and left pleura. This constellation of findings is consistent with a subacute stage of pericardial and pleural inflammation in the setting of post cardiac injury syndrome.
Treatment of PCIS consists on anti-inflammatory therapy (Class I-B recommendation), similar to the treatment of acute pericarditis. Perioperative prophylaxis has also previously been explored. A meta analysis of 894 patients6 evaluated the role of colchicine, methylprednisolone and aspirin compared to placebo for primary prevention of PPS and their results showed that only colchicine was associated to decreased risk for PPS [OR 0.38, 0.22-0.65] albeit with increased reported GI side effects.
Furthermore, the colchicine for prevention of post-pericardiotomy syndrome (COPPS and COPPS-2)7,8 trials confirmed the efficacy of preventive colchicine specifically for PPS with a number needed to treat (NNT) of 8 and 10 respectively. ESC guidelines recommend colchicine 0.5mg twice daily 3 days before and 1 month after surgery (Class II-A). Noteworthy, however, colchicine is not currently recommended for post-operative effusions without signs of systemic inflammation, and neither are NSAIDs; an importance nuance to be mindful of.2,3
Our patient was discharged on colchicine 0.6mg twice daily indefinitely and ibuprofen 600mg three times daily for 4 weeks. He did not experience significant improvement with ibuprofen and was transitioned to a 2-week course of prednisone 40mg daily followed by a taper. Glucocorticoid administration is usually required for a minority of patients with contraindications for aspirin and NSAIDs or in case of refractory symptoms, and it should always be tapered before colchicine is stopped.3 Steroids are not usually the initial treatment and are typically reserved for patients who fail initial treatment (colchicine and NSAIDs).2,5 In fact, high-dose steroids (1mg/kg) were shown to be associated with higher risk of recurrences compared to low-dose (0.2-0.5 mg/kg), in a retrospective study of 100 patients with recurrent pericarditis published in 2008.9
Lastly, given our patient's history of both Graves' disease and multiple sclerosis, the possibility of propensity to PCIS in patients with other autoimmune diseases was also considered. Further studies should be designed addressing the incidence of PPS in this population, to support use of preventive therapy.
References
Lehto J, Kiviniemi T, Gunn J, Airaksinen J, Rautava P, Kytö V. Occurrence of postpericardiotomy syndrome: association with operation type and postoperative mortality after open-heart operations. J Am Heart Assoc 2018;7:e010269.
Adler Y, Charron P, Imazio M, et al. 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: The European Association for Cardio‐Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921–64.
Chetrit M, Xu B, Kwon DH, et al. Imaging-guided therapies for pericardial diseases. JACC Cardiovasc Imaging 2019;pii:S1936-878X;30879-4. [Epub ahead of print]
Imazio M, Brucato A, Markel G, et al. Meta-analysis of randomized trials focusing on prevention of the postpericardiotomy syndrome. Am J Cardiol 2011;108:575-9.
Imazio M, Trinchero R, Brucato A, et al. COlchicine for the Prevention of the Post-pericardiotomy Syndrome (COPPS): a multicentre, randomized, double-blind, placebo-controlled trial. Eur Heart J 2010;31:2749-54.
Imazio M, Brucato A, Ferrazzi P, et al. Colchicine for Prevention of postpericardiotomy syndrome and postoperative atrial fibrillation: the COPPS-2 randomized clinical trial. JAMA 2014;312:1016-23.
Imazio M, Brucato A, Cumetti D, et al. Corticosteroids for recurrent pericarditis: high versus low doses: a nonrandomized observation. Circulation 2008;118:667–71.