A 33-year-old male, history of congenitally corrected transposition of the great vessels, bicuspid aortic stenosis (status post valvotomy, homograft, and ultimately mechanical valve replacement) complicated by complete heart block (status post pacemaker with upgrade to defibrillator in the setting of reduced ventricular function) and atrial tachycardia, initially presented for further evaluation due to 15 months of persistent shortness of breath and right-sided chest/abdominal pain. Patient had already undergone extensive diagnostic cardiovascular workup over a 6-month course, between his local hospital and our institution, due to his symptoms.
Left and right heart catheterization was negative for obstructive coronary artery disease or significant valvulopathies but noted mild to moderate biventricular combined systolic and diastolic dysfunction on ventriculogram with the illustrated hemodynamics (Figure 1).
Figure 1
Figure 1
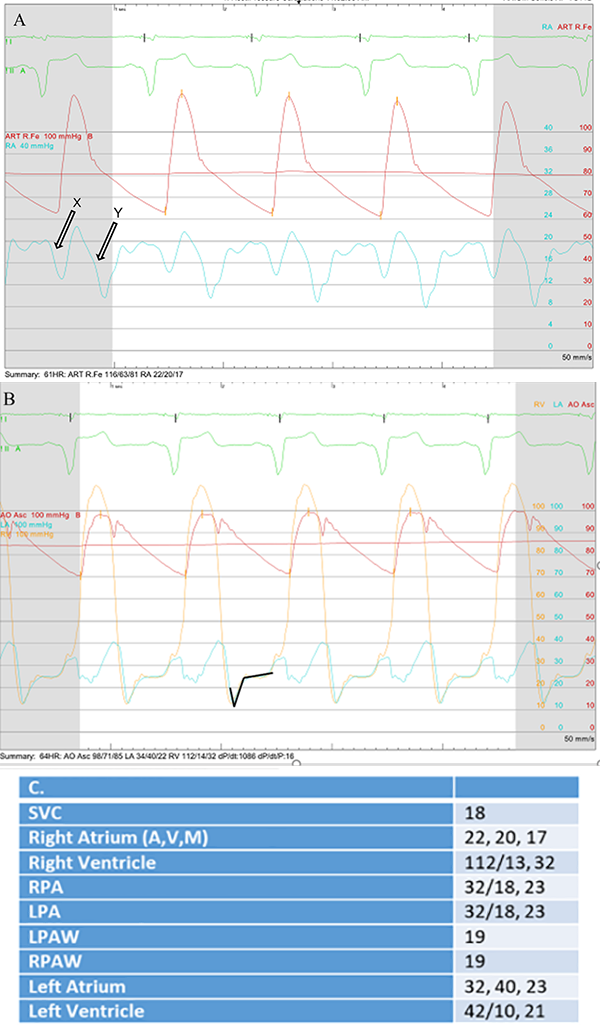
Figure 1: Hemodynamic findings in our patient. A) Mean right atrial pressure is elevated with prominent x and y descents (arrows). B) Systemic (morphologic right) ventricle and left atrial diastolic waveforms both manifest "dip and plateau" (square root sign) leading to elevated and equalized filling pressures. C). Pressures as determined by catheterization.
*Estimated RA pressure was (mean) of 17 mmHg and LA pressure is estimated to be 23 (mean). LV/RV pressures are reported as SBP/DBP and end diastolic pressures.
Figure 1: Hemodynamic findings in our patient. A) Mean right atrial pressure is elevated with prominent x and y descents (arrows). B) Systemic (morphologic right) ventricle and left atrial diastolic waveforms both manifest "dip and plateau" (square root sign) leading to elevated and equalized filling pressures. C). Pressures as determined by catheterization.
*Estimated RA pressure was (mean) of 17 mmHg and LA pressure is estimated to be 23 (mean). LV/RV pressures are reported as SBP/DBP and end diastolic pressures.
Liver biopsy, performed due to intermittent ascites, showed normal hepatic architecture with mild patchy centrilobular sinusoidal dilatation and congestion, without any signs of cirrhosis. Computed tomography (CT) chest scan (Figure 2) showed a 10 x 3 x 1.6 cm loculated pericardial effusion running vertically and overlying the anterior atrioventricular groove with distortion of the base of the anterior, morphologic left ventricle, as well as mild to moderate calcifications involving the visceral pericardium.
Figure 2
Figure 2
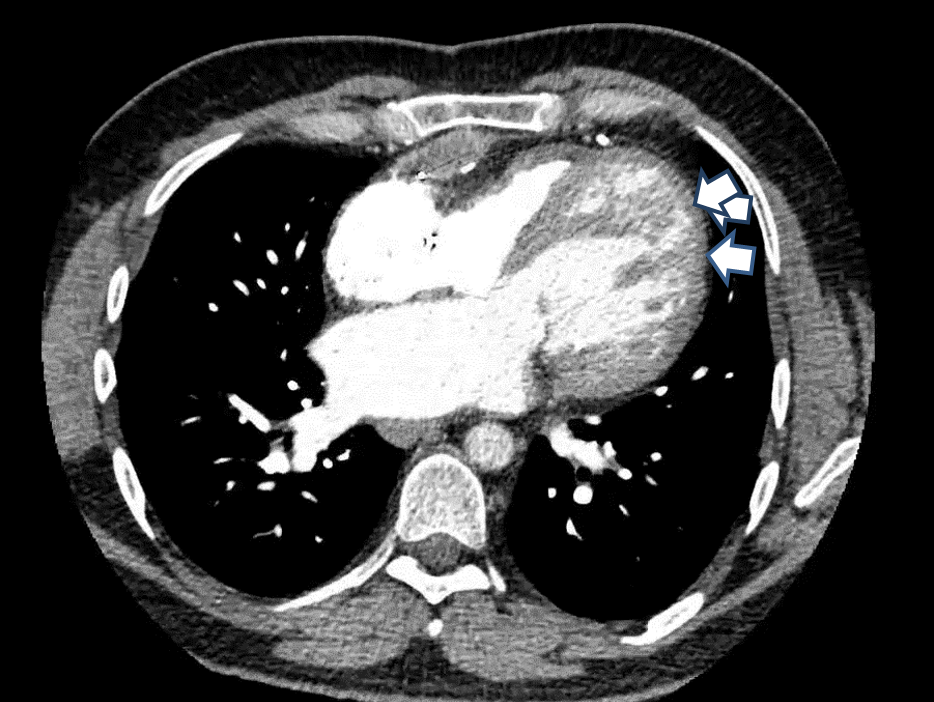
Figure 2: CT chest scan demonstrating a pericardial effusion with distortion/compression of the base of the anterior (morphologic left) ventricle. Mild to moderate thickening involving the visceral pericardium was also noted (arrows).
Figure 2: CT chest scan demonstrating a pericardial effusion with distortion/compression of the base of the anterior (morphologic left) ventricle. Mild to moderate thickening involving the visceral pericardium was also noted (arrows).
Given the above findings, patient was referred to pericardial disease clinic for our opinion regarding further management. Repeat transthoracic echocardiogram was done, showing mildly dilated systemic ventricle with hypertrophy and mildly decreased systolic function (ejection fraction [EF] 45%); well-positioned aortic prosthesis without regurgitation and stable peak/ mean gradients 36/20 mm Hg; normal subpulmonic ventricle with 1-2+ atrioventricular valve insufficiency; small pericardial effusion; septal bounce; and these additional findings (Figure 3).
Figure 3
Figure 3
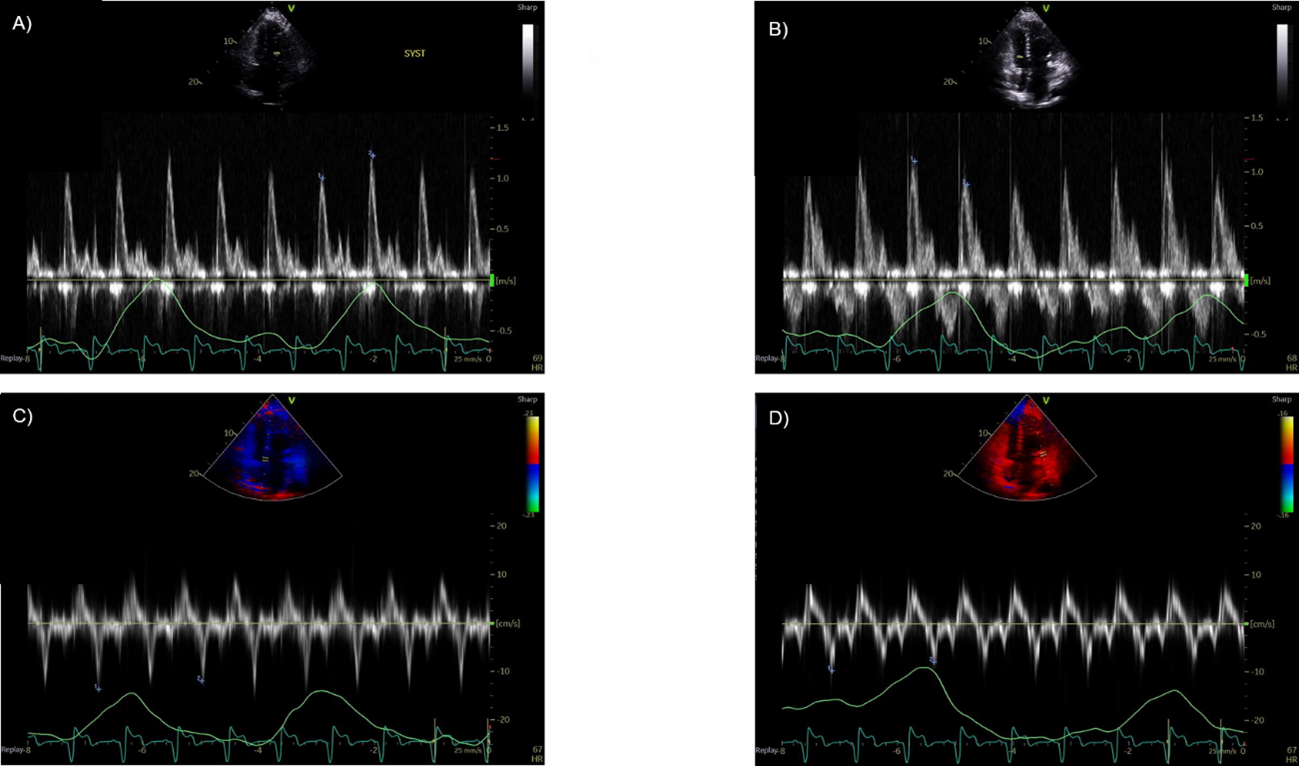
Figure 3: A) and B) demonstrating signs of respiratory variation of the mitral valve (18%) and tricuspid valve (-25%) inflows. This is suggestive of restrictive disease. C) and D) echo showing annulus reversus suggestive of constriction.
Figure 3: A) and B) demonstrating signs of respiratory variation of the mitral valve (18%) and tricuspid valve (-25%) inflows. This is suggestive of restrictive disease. C) and D) echo showing annulus reversus suggestive of constriction.
Which of the following is the most accurate statement regarding the diagnosis in this patient?
Show Answer
The correct answer is: F. Mixed Constrictive and Restrictive Disease
Several etiologies for cardiomyopathy can coexist. Our patient's presentation with initial symptoms of dyspnea and intermittent ascites (later proven to be hepatic congestion on liver biopsy) is likely secondary to right heart failure. This raises the suspicion for constrictive pericarditis, especially in the setting of these objective findings on multimodality evaluation: visceral pericardial calcifications on CT chest scan, increased atrial pressure with prominent x and y-descents, equalization of end-diastolic pressures in the chambers, and dip-and-plateau or square root sign of ventricular diastolic pressure on invasive angiography.1 The etiology for constriction in our patient is attributed possibly to prior surgical interventions and prior sternotomies during early childhood.
However, some clinical and hemodynamic features can be nonspecific and be similar between pericardial diseases and cardiomyopathies. Thus, echocardiography is important to evaluate for respiratory variation in ventricular filling, interventricular dependence, and augmented longitudinal motion of the heart. Prior studies have identified dissociation between intrathoracic and intracardiac pressures that result in abnormal septal movement as hallmark signs of constriction.2-5 Our patient expectedly had signs of septal bounce and associated annulus reversus that were suggestive of constriction. However, he also exhibited delayed ventricular relaxation, as demonstrated by the decreased mitral annular e' velocities.6-8 Furthermore, the presence of tricuspid regurgitation, mild hypertrophy with decreased EF, and elevated left ventricular end-diastolic pressure (LVEDP) on cardiac catheterization were suggestive of the concomitant presence of an underlying myocardial dysfunction in the setting of mixed constrictive and restrictive disease, making this case atypical.
Discriminating the entity of mixed physiology from pure constriction is essential due to the prognostic implications. Yamada et al. first investigated this in 38 patients with mixed constrictive and restrictive physiology who met inclusion criteria (localized thickening of pericardium on echo with confirmation by magnetic resonance imaging or CT; restrictive Doppler findings of transmitral and/or pulmonary venous flow velocity patterns; no significant respiratory variations on early diastolic transmitral flow velocity <25%) and found that this unique group had high mortality and poorer long term clinical outcomes.8 Additionally Yang et al. were able to determine that in constriction, patients with higher right atrial/pulmonary arterial wedge pressures (RA/PAWP) were more likely to be associated with pure isolated constriction.9 They also identified that patients with RA/PAWP ˃0.77 (our patient's RA/PAWP was 0.89) had significantly higher survival rates.9
Returning to our patient, given his extensive prior surgical history and clinical status, he was further optimized medically with initiation of loop diuretics (no clear indication for anti-inflammatory agents) and recommended close monitoring, with plans for pericardiectomy in the future if worsening occurs.
References
Sorajja P. Invasive hemodynamics of constrictive pericarditis, restrictive cardiomyopathy, and cardiac tamponade. Cardiol Clin 2011;29:191-99.
Hatle LK, Appleton CP, Popp RL. Differentiation of constrictive pericarditis and restrictive cardiomyopathy by Doppler echocardiography. Circulation 1989;79:357-70.
Oh JK, Hatle LK, Seward JB, et al. Diagnostic role of Doppler echocardiography in constrictive pericarditis. J Am Coll Cardiol 1994;23:154-62.
Welch TD, Ling LH, Espinosa RE, et al. Echocardiographic diagnosis of constrictive pericarditis: Mayo Clinic criteria. Circ Cardiovasc Imaging 2014;7:526-34.
Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 2016;29:277-314.
Qamruddin S, Alkharabsheh SK, Sato K, et al. Differentiating constriction from restriction (from the Mayo Clinic Echocardiographic Criteria). Am J Cardiol 2019;124:932-38.
Yamada H, Tabata T, Jaffer SJ, et al. Clinical features of mixed physiology of constriction and restriction: echocardiographic characteristics and clinical outcome. Eur J Echocardiogr 2007;8:185-94.
Yang, JH, Miranda WR, Borlaug, BA, et al. Right atrial/pulmonary arterial wedge pressure ratio in primary and mixed constrictive pericarditis. J Am Coll Cardiol 2019;73:3312-21.