A 54-year-old man with a recent diagnosis of intermediate risk was referred to the cardio-oncology clinic for cardiac assessment. He was due to receive consolidation with a regimen potentially including anthracyclines and, if suitable, allogeneic hematopoietic stem cell transplantation (HSCT) from a human leukocyte antigen–identical sibling donor. He had already completed induction therapy with idarubicin, cytarabine (classical 3+7), and midostaurin, achieving hematological complete remission.
His medical history includes hypertension, hypercholesterolemia, and coronary artery disease (CAD). His only coronary event was a non–ST-segment elevation myocardial infarction 15 years earlier that required percutaneous coronary intervention of the proximal right coronary artery (no other coronary lesions were present). His left ventricular ejection fraction (LVEF) at his most recent (6 months earlier) follow-up appointment was 55%, and exercise stress test findings at that time were clinically and electrically negative.
Cardiac Assessment and Investigations
His current medications include omeprazole 20 mg OID, enalapril 20 mg BID, aspirin 100 mg OID, carvedilol 12.5 mg BID, rosuvastatin 20 mg OID, and acyclovir 400 mg BID. He is physically active, free of symptoms from a cardiac viewpoint, and capable of performing activities equivalent to >4 METs per day, globally self-reporting himself in New York Heart Association (NYHA) class I and Canadian Cardiovascular Society (CCS) class I.
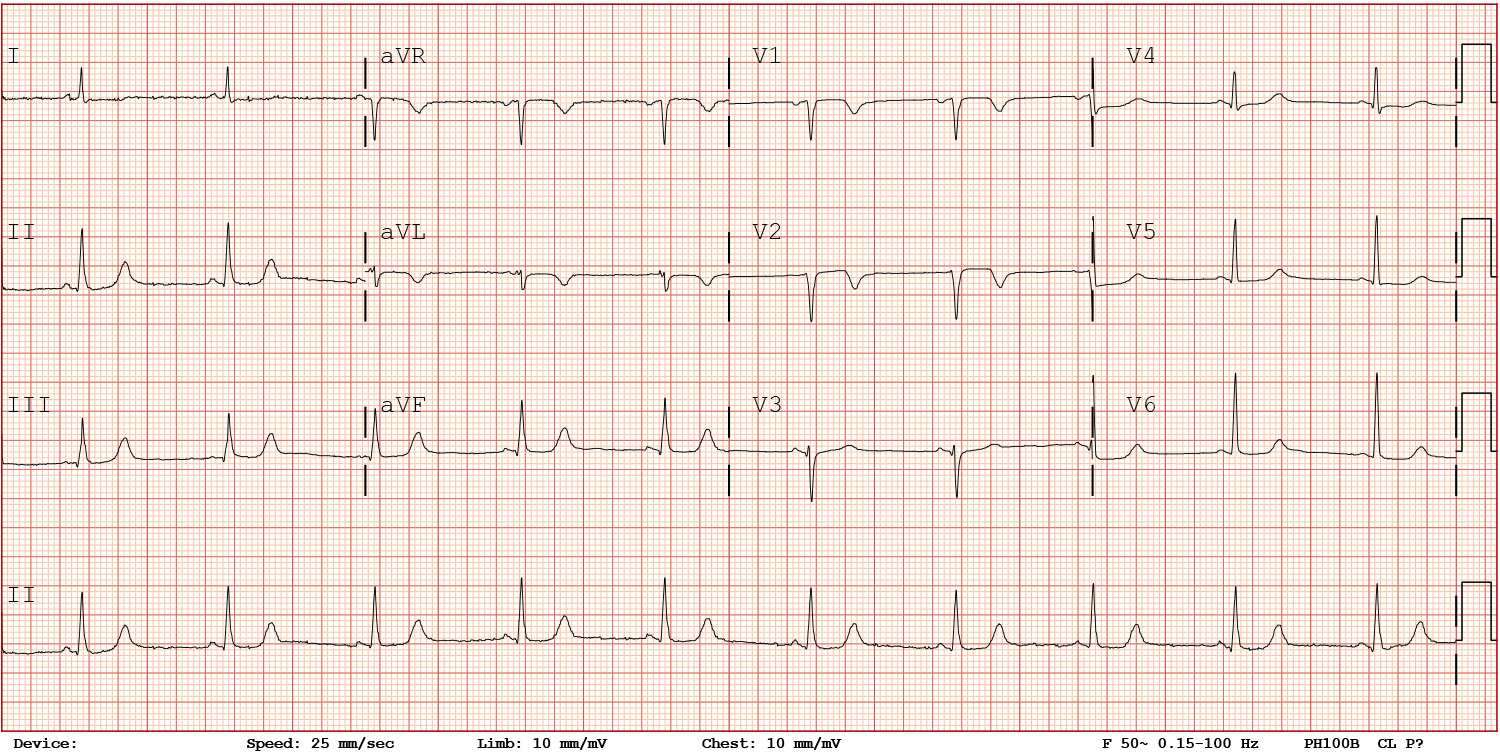
Physical examination findings are unremarkable, including blood pressure (BP) 110/76 mm Hg and heart rate 65 bpm. An electrocardiogram (ECG) shows sinus rhythm with a normal P-R interval, a narrow QRS complex, Q waves in leads V1 and V2, and inversion of the T wave in leads V1, V2, and aVL with other repolarization abnormalities (Figure 1). Laboratory tests include kidney function test values and electrolyte levels within the reference ranges, total cholesterol level 240 mg/dL, low-density lipoprotein cholesterol level 70 mg/dL, fasting plasma glucose level 97 mg/dL, hemoglobin A1c (HbA1c) concentration 5.6%, hemoglobin level 12 g/dL, and iron and thyroid profiles within the reference ranges. Cardiac biomarker levels have not been assessed recently.
Figure 1
Figure 1
Which one of the following approaches to minimize cardiac risk with HSCT is most in line with the current available evidence?
Show Answer
The correct answer is: C. NT-proBNP assay and transthoracic echocardiography (TTE) performed; if LVEF is unremarkable and no other cardiac abnormalities are detected, proceed with HSCT.
In accordance with the recommendations (based on expert opinion) outlined in the 2022 Guidelines on Cardio-Oncology issued by the European Society of Cardiology (ESC) in collaboration with the European Hematology Association (EHA) and the International Cardio-Oncology Society (IC-OS),1 this patient underwent TTE and NT-proBNP level assessment. Given that he had received an induction regimen involving idarubicin and was planned to receive further anthracyclines during consolidation, measurement of his hs-cTn I level was requested.
Echocardiographic windows were poor and showed a nondilated left ventricle (LV) with an estimated mild (LVEF 50%) impairment of systolic function (Video 1). Regional wall motion abnormalities could not be reliably evaluated because of the poor image quality. However, diastolic function was normal, as was size and function of the right ventricle. No significant valve disease or signs of pulmonary hypertension were noted.
Video 1
Because of the suboptimal sonographic window and the importance of accurately evaluating and documenting systolic function in all patients being considered for HSCT, a CMR was requested. Stress pharmacological testing using regadenoson was performed. The stress CMR revealed LVEF 54% (mildly impaired systolic function; normal LVEF >57% on CMR) with no inducible ischemia (Video 2). Hs-cTn and NT-proBNP levels were within the reference ranges; on the basis of these findings, the patient was deemed eligible for HSCT from a cardiac viewpoint. To further optimize the medical management of his cardiac comorbidities, the doses of the beta-blocker and statin were increased, and ezetimibe was added.
Video 2
He underwent allogeneic HSCT with a reduced-intensity conditioning regimen based on busulfan and fludarabine. Graft-versus-host prophylaxis was administered with tacrolimus, sirolimus, and mycophenolate mofetil. At the time of this report (3 months post transplantation), he had been reviewed in the cardio-oncology clinic and had an uneventful recovery/course without any significant complications.
HSCT, commonly known as "bone marrow transplantation," is a well-established and life-saving treatment for high-risk hematological neoplasm and nonmalignant entities (leukemias, lymphomas, hemoglobinopathies, bone marrow failure syndromes, and primary immune deficiencies) and for some solid tumors or metabolic diseases. Every year, >20,000 patients undergo HSCT and approximately 43,000 patients receive this treatment in Europe, according to the European Society for Blood and Marrow Transplantation (EBMT) annual reports.2,3
The overall incidence of early cardiotoxic events following HSCT ranges from 5% to 20% among recipients of HSCT, with common complications including atrial tachyarrhythmias and fluid overload.4 In the long term, up to 22% of patients may experience an adverse event, primarily characterized by a decline in LVEF to <45%.5 As HSCT is now increasingly offered to older adults, pre-existing cardiovascular (CV) conditions should be controlled because these are related to an increase in transplant-related mortality, according to the Hematopoietic Cell Transplantation-Comorbidity Index (HCT-CI).6-8
A thorough CV evaluation has now become a core element of pretransplantation assessment. This evaluation occurs in the hematology clinic, with referral to a cardio-oncology clinic for patients at higher risk. The aim is to optimize the management of CV disease while stratifying the individual risk of cardiotoxicity.1 Furthermore, baseline CV risk stratification assists the hematology team in tailoring the conditioning regimens for HSCT, allowing them to choose between the high-intensity, myeloablative conditioning regimens and less-toxic, reduced-intensity protocols.4,7
The presence of one or more of the following major factors categorizes the patients into a group at high risk of developing CV complications in the context of HSCT: 1) the type of HSCT (higher in the case of allogenic); 2) pre-existing CV risk factors and/or comorbidities (arrhythmias, CAD, moderate-to-severe valvular heart disease, and heart failure [HF] or LVEF <50%); 3) exposure to cardiotoxic anticancer therapies received before and during HSCT (alkylating agents, induction with anthracyclines or conditioning with high-dose cyclophosphamide and total body irradiation, mediastinal radiation therapy, or mantle field radiation); and 4) development of graft-versus-host disease (GVHD).1,9,10 Moreover, the use of immunosuppressive therapy for the prevention and management of GVHD, such as corticosteroids and calcineurin inhibitors, increases the likelihood of developing hypertension, dyslipidemia, insulin resistance, and metabolic syndrome, both in the short term and long term. Additionally, novel treatments for GVHD, such as ibrutinib and ruxolitinib, have also been associated with the development of CV risk factors and occurrence of cardiac events, including hyperlipidemia and atrial fibrillation.7,11
Importantly, stem cell transplantation can still be successfully carried out in those with LVEF <50% in a select group of patients.
CV complications are increasingly being recognized as an important morbidity of HSCT.5,7,10 This recognition has led to the development of several risk predictors.6,8 These have been synthetized in the recommendations put forward in the ESC and IC-OS guidelines. The evidence base is limited at present; the guidelines are reflective of this and include many expert consensus recommendations.
The ESC and IC-OS guidelines recommend CV assessment for all patients prior to HSCT, including a comprehensive medical history, physical examination, body mass index calculation, HR and BP measurement, fasting blood glucose assay, lipid profile, and HbA1c concentration determination. In addition, ECG and TTE are recommended in all cases, as is measuring baseline natriuretic peptide (NP) levels. The use of CPET in select patients at high risk is also mentioned, although further validation is needed to determine its role in better stratifying the risk of cardiotoxicity and predicting future CV outcomes in this population.1
There are limited data on the role of cardioprotection to prevent cardiotoxicity in the HSCT population. A small, open-label study without a placebo arm (the OVERCOME [preventiOn of left Ventricular dysfunction with Enalapril and caRvedilol in patients submitted to intensive ChemOtherapy for the treatment of Malignant hEmopathies] study) investigated the impact of combining angiotensin-converting enzyme inhibitors and beta-blockers in 90 HSCT patients without pre-existing LV systolic dysfunction.12 Patients were monitored for 6 months after transplantation; the intervention group did not experience a significant reduction in LVEF and had a lower incidence of the combined event of death or HF than did the control group. However, the widespread applicability of this study to clinical practice may be challenging, and larger randomized control trials are required.
Due to the elevated risk of late-effect cardiotoxicity in this cohort, CV surveillance is recommended in survivors of HSCT. A comprehensive clinical assessment, including physical examination, BP measurement, lipid profile evaluation, and HbA1c concentration determination, is recommended in the ESC and IC-OS guidelines at 3 months and 1 year after transplantation, and annually thereafter. The use of imaging techniques and cardiac biomarker analyses should be determined on the basis of the individual patient's risk profile. TTE and NP level measurements are recommended for patients at low risk if new cardiac symptoms arise. In patients at high risk, both tests are recommended at 3 and 12 months post HSCT as part of early surveillance.1 However, the frequency and nature of monitoring remain up for debate to ensure that surveillance programs are both cost-effective and able to detect CV late effects at an early stage.
References
Lyon AR, López-Fernández T, Couch LS, et al. 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J 2022;43:4229-361.
D'Souza A, Fretham C, Lee SJ, et al. Current use of and trends in hematopoietic cell transplantation in the United States. Biol Blood Marrow Transplant 2020;26:e177-e182.
Passweg JR, Baldomero H, Ciceri F, et al. Hematopoietic cell transplantation and cellular therapies in Europe 2021. The second year of the SARS-CoV-2 pandemic. A report from the EBMT Activity Survey. Bone Marrow Transplant 2023;58:647-58.
Majhail NS. How to perform hematopoietic stem cell transplantation. JACC CardioOncol 2021;3:742-6.
Auberle C, Lenihan D, Gao F, Cashen A. Late cardiac events after allogeneic stem cell transplant: incidence, risk factors, and impact on overall survival. Cardiooncology 2023;9:1.
Sorror ML, Giralt S, Sandmaier BM, et al. Hematopoietic cell transplantation specific comorbidity index as an outcome predictor for patients with acute myeloid leukemia in first remission: combined FHCRC and MDACC experiences. Blood 2007;110:4606-13.
López-Fernández T, Vadillo IS, de la Guía AL, Barbier KH. Cardiovascular issues in hematopoietic stem cell transplantation (HSCT). Curr Treat Options Oncol 2021;22:51.
Vasbinder A, Hoeger CW, Catalan T, et al. Cardiovascular events after hematopoietic stem cell transplant: incidence and risk factors. JACC: CardioOnc 2023;Sep 19:[ePub ahead of print].
Oliveira GH, Al-Kindi SG, Guha A, Dey AK, Rhea IB, deLima MJ. Cardiovascular risk assessment and management of patients undergoing hematopoietic cell transplantation. Bone Marrow Transplant 2021;56:544-51.
Rotz SJ, Ryan TD, Hayek SS. Cardiovascular disease and its management in children and adults undergoing hematopoietic stem cell transplantation. J Thromb Thrombolysis 2021;51:854-69.
Ohmoto A, Fuji S. Cardiac complications associated with hematopoietic stem-cell transplantation. Bone Marrow Transplant 2021;56:2637-43.
Bosch X, Rovira M, Sitges M, et al. Enalapril and carvedilol for preventing chemotherapy-induced left ventricular systolic dysfunction in patients with malignant hemopathies: the OVERCOME trial (preventiOn of left Ventricular dysfunction with Enalapril and caRvedilol in patients submitted to intensive ChemOtherapy for the treatment of Malignant hEmopathies). J Am Coll Cardiol 2013;61:2355-62.