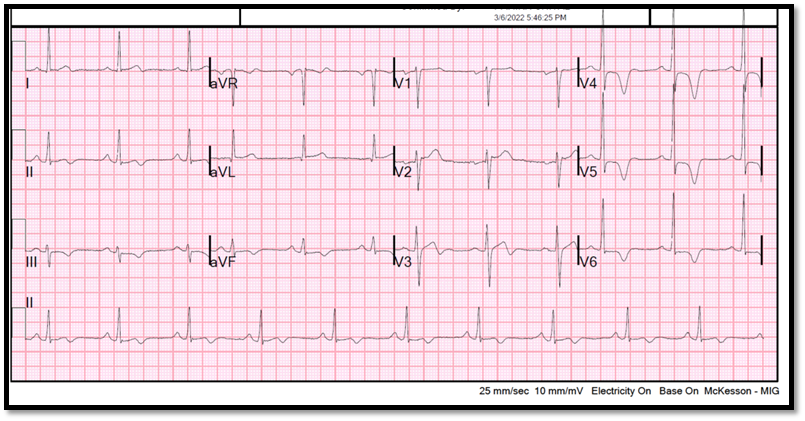
A 50-year-old man of Hispanic background with past medical history of hypertension and dyslipidemia presents to the emergency department with intermittent chest pain and an abnormal electrocardiogram (ECG) (Figure 1).
Figure 1: Sinus rhythm with left ventricular hypertrophy and deep symmetric T wave inversion in the lateral leads
Figure 1
He has no known family history of cardiovascular disease. Blood pressure is 143/83 mmHg and heart rate is 67 bpm. The patient's echocardiogram shows normal biventricular function without wall motion abnormalities. Serial troponin I levels are negative and coronary computed tomography angiography (CTA) demonstrates normal coronary arteries (Coronary Artery Disease Reporting and Data System [CAD-RADS] 0). Given ECB abnormalities, a cardiovascular magnetic resonance (CMR) is ordered for further characterization (Figures 2,3, and Video 1).
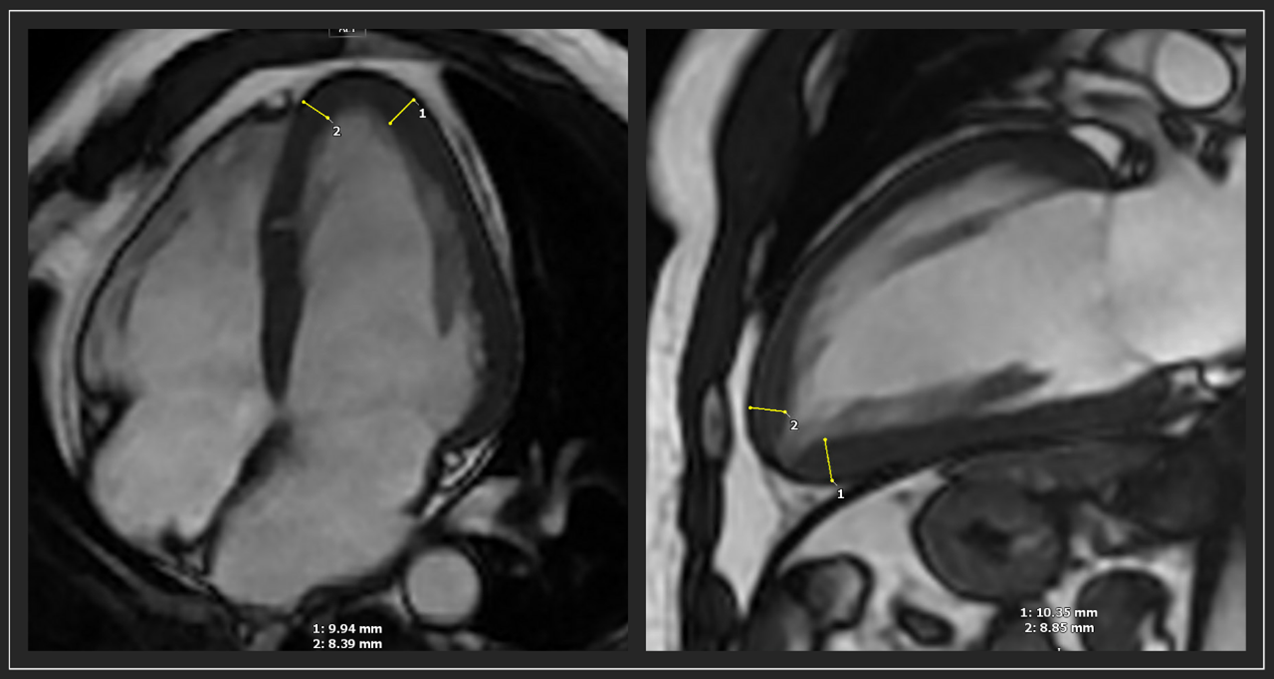
Figure 2: End-diastolic fast imaging employing steady-state acquisition (FIESTA) images showing the lack of wall thickness tapering from basal to apical segments
Figure 2
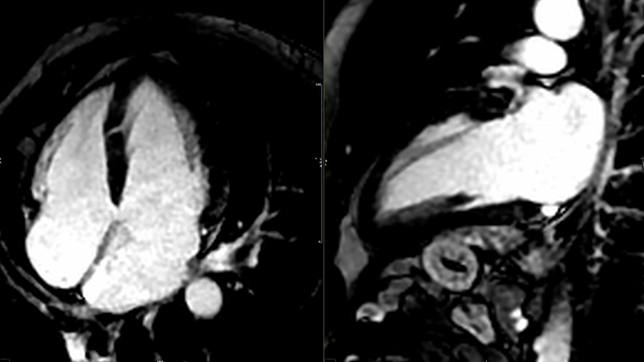
Figure 3: Late gadolinium enhancement images showing the absence of myocardial uptake (normal pattern)
Figure 3
Video 1: Long axis Cine FIESTA
Video 1
Considering the CMR findings, what is the most appropriate next step in this patient's care?
Show Answer
The correct answer is: C. Refer patient to hypertrophic cardiomyopathy clinic.
Hypertrophic cardiomyopathy (HCM) is an umbrella term for a genetic disorder characterized by left ventricular hypertrophy unexplained by loading conditions. Even in the absence of absolute hypertrophy or any wall segment meeting the guideline criteria1 for HCM (≥15 mm), this patient shows a lack of segmental thickness tapering towards the apex with some apical segments measuring up to 10 mm. As the normal heart exhibits tapering of wall thickness towards the apex, loss of this pattern is abnormal.2,3 Relative apical HCM (ApHCM) may represent an early disease phenotype that may eventually progress to overt ApHCM.3 It has been shown that apical stress perfusion defects (or inducible ischemia) are a universal feature of ApHCM and relative ApHCM, possibly explaining the common chest pain presentation in these patients.4 Recently, new criteria for the diagnosis of ApHCM have been proposed using body surface area (BSA) indexed cut-offs. In the United Kingdom-based study a maximum apical >5.2 to 5.6 mm/m2 identified ApHCM patients (vs. healthy volunteers) with an accuracy of 0.94.5 However, one of the main limitations was the lack of representation of different races/ethnicities with >98% of the subjects being British White. Regarding sex differences, as expected, wall thickness for all segments was higher for men (2 mm on average) but there was no clinically significant numerical difference when indexed to BSA.
Answer choice A is incorrect. ECG is clearly abnormal and CMR findings provide a plausible explanation.
Answer choice B is incorrect. ECG findings in this patient relate to ApHCM and not Wellens syndrome. A negative coronary CTA has a high negative predictive value for obstructive CAD.
Answer choice D is incorrect. There is no need to adjust hypertension regimen since blood pressure is currently controlled and left ventricular hypertrophy is not caused by hypertensive heart disease.
References
Ommen SR, Mital S, Burke MA, et al. 2020 AHA/ACC guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020;76:3022-55.
Hughes RK, Knott KD, Malcolmson J, et al. Apical hypertrophic cardiomyopathy: the variant less known. J Am Heart Assoc 2020;9:e015294.
Flett AS, Maestrini V, Milliken D, et al. Diagnosis of apical hypertrophic cardiomyopathy: T-wave inversion and relative but not absolute apical left ventricular hypertrophy. Int J Cardiol 2015;183:143–48.
Hughes RK, Augusto JB, Knott K, et al. Apical ischemia Is a universal feature of apical hypertrophic cardiomyopathy. Circ Cardiovasc Imaging 2023;16:e014907.
Hughes RK, Shiwani H, Rosmini S, et al. Improved diagnostic criteria for apical hypertrophic cardiomyopathy. JACC Cardiovasc Imaging 2023;Sep 29:[EPub ahead of print].