

Discordance Between Coronary Artery Calcium Area and Density Predicts Long-Term Atherosclerotic Cardiovascular Disease Risk
Introduction
Current American College of Cardiology (ACC)/American Heart Association(AHA)1 and European Society of Cardiology (ESC) guidelines2 recommend coronary artery calcium (CAC) measurement via gated non-contrast computed tomography (CT) as the strongest established imaging modality to help guide atherosclerotic cardiovascular disease (ASCVD) risk assessment and the initiation of preventive pharmacotherapy, particularly among primary prevention patients aged 40-79 years who have an intermediate 10-year ASCVD risk. While CAC is closely associated with ASCVD risk, there may be considerable heterogeneity in plaque morphology among individuals with similar CAC burden, which could differentially influence long-term ASCVD outcomes3 and the approach to risk reduction.
The Agatston method, the most widely used CAC scoring algorithm, is defined as the product of plaque area and a quantized peak calcium density weighting factor for each lesion, the latter of which is summed across all lesions to provide a total CAC score. Calcium density is measured radiologically as the plaque attenuation on non-contrast CT in Hounsfield Units and measures the concentration of calcium within a given atherosclerotic plaque. Though calcium density is positively associated with both chronological age and the biological age of plaque, calcium density is inversely associated with traditional ASCVD risk factor burden and lesion vulnerability when accounting for calcium area. These results suggest that calcium density cannot be interpreted independent from calcium area, and that the surface area of the plaque is likely the predominant driver of heightened risk among individuals with high Agatston CAC scores.4 Whether discordance between calcium area and density has long-term prognostic importance in ASCVD risk remains unknown.
Methods
We studied 10,373 primary prevention patients from the CAC consortium with prevalent CAC who were physician-referred to undergo cardiac CT. Mean calcium density and plaque area were categorized as high (above the median for the study sample) or low (below the median for the study sample). Next, participants were divided into quartiles of four mutually exclusive concordant/discordant groups: low/low (less than the median for both mean calcium density and calcified plaque area), high/low (greater than or equal to the median for mean calcium density and less than the median for calcified plaque area), low/high (less than the median for mean calcium density and greater than or equal to median for calcified plaque area), and high/high (greater than or equal to median for both mean calcium density and calcified plaque area). Cox proportional hazards regression assessed the association of calcium area/density groups with ASCVD mortality, adjusting for traditional risk factors and the total Agatston CAC score.
Results
The mean age was 56.7 years old and 24% were female (Table 1).
Table 1

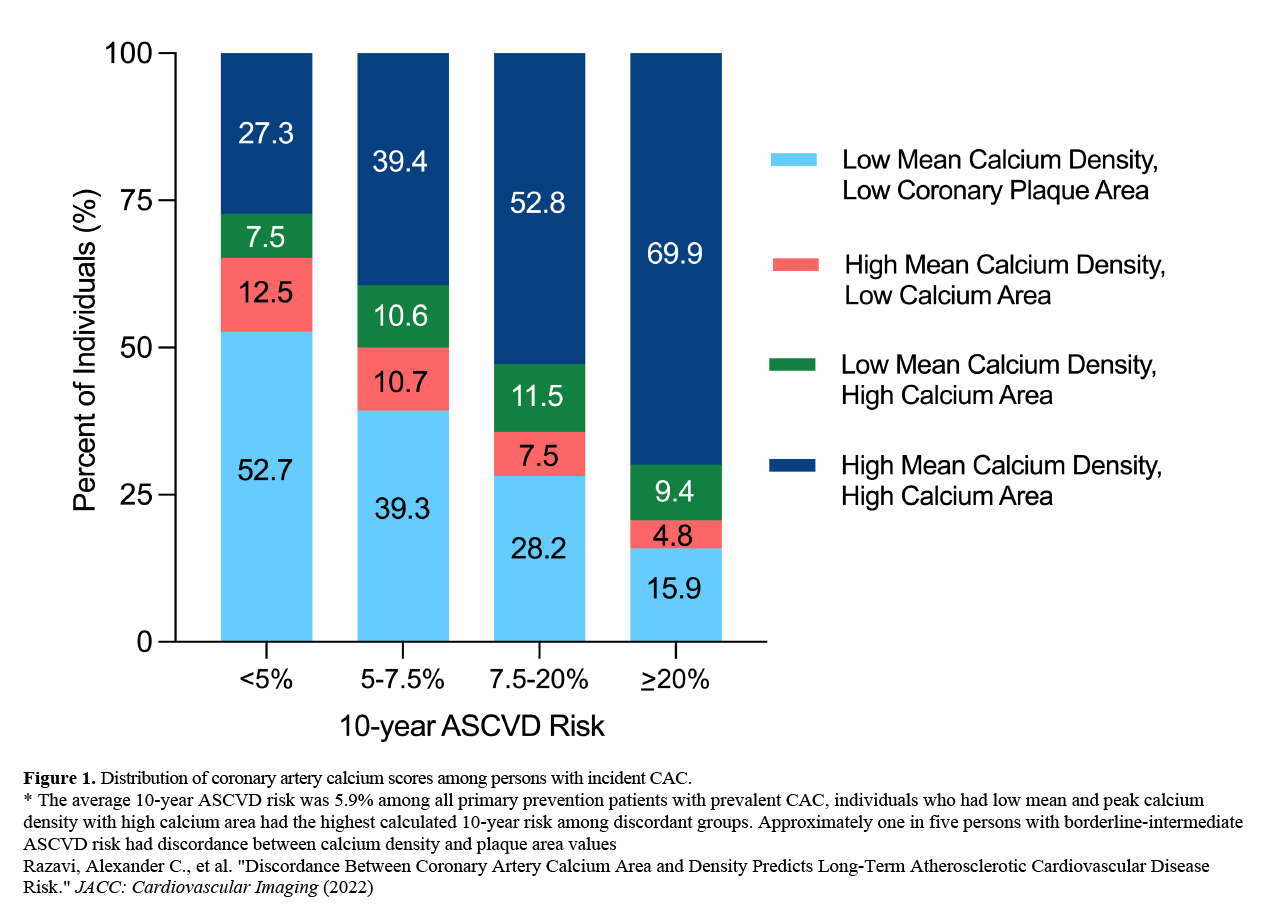
The prevalence of plaque discordance was 19% (9% low calcium area-high calcium density, 10% high calcium area-low calcium density) (Figure 1).
Figure 1
A total of 197 ASCVD deaths occurred over a median follow-up period of 11.7 years. The distribution of ASCVD deaths differed among the four groups with similar event rates observed for individuals with high mean calcium density/low calcium area (0.3 per 1,000 person years) and low mean calcium density/low calcium area (0.8 per 1,000 person years) versus the ASCVD mortality rates of 2.3 and 2.8 events per 1,000 person years for the low mean calcium density/high calcium area and high mean calcium density/high calcium area groups, respectively. Female sex (OR=1.48, 95% CI: 1.27-1.74) and body mass index (BMI) (OR=0.81, 0.76-0.87, per 5 kg/m2 higher) significantly associated with high calcium density discordance, whereas diabetes mellitus (OR=2.23, 95% CI: 1.85-3.19) was most strongly associated with discordantly low calcium density (Table 2).
Table 2

Over a median of 11.7 years (Figure 2), compared to those with low calcium area-low calcium density, individuals with low calcium area-high calcium density had a 71% lower risk of ASCVD death (HR=0.29, 95% CI: .09-0.95) (Table 3). By contrast, the concordant high calcium area and mean calcium density phenotype was associated with a 50% (HR=1.50, 95% CI: 1.01, 1.26) higher ASCVD mortality risk, though was not significant when considering the Agatston CAC score.
Figure 2
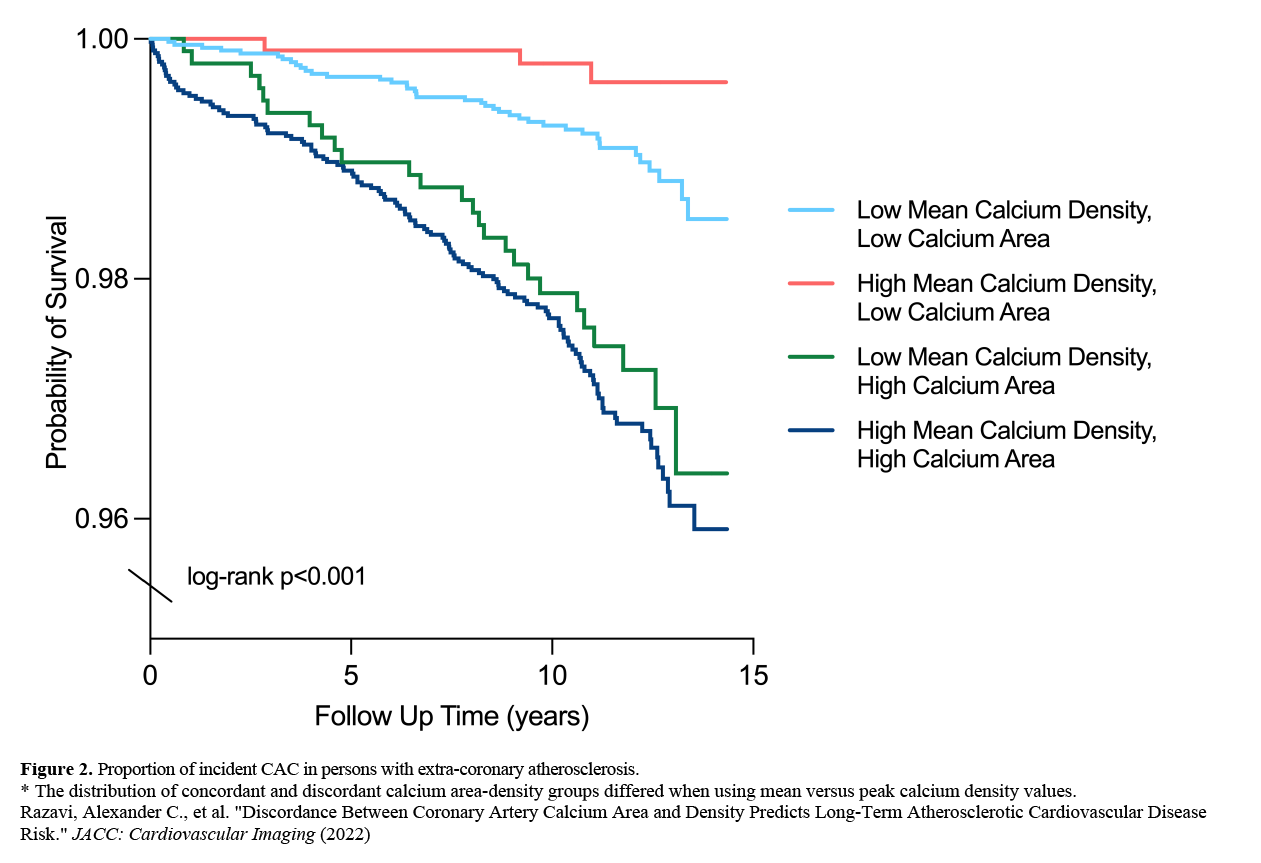
Table 3

Discussion
In a sample of physician-referred primary prevention patients who underwent CAC scanning, we defined groups that placed approximately one-fifth of persons with prevalent CAC into phenotypes characterized by calcium area-density discordance. Furthermore, CAC area-density groups were associated with different risk factor burden, as lower BMI, normal blood pressure, and the absence of a family history of congenital heart disease (CHD) conferred a higher likelihood for the low calcium area-high calcium density phenotype, whereas all modifiable risk factors except for cigarette smoking were positively associated with high calcium area and low calcium density. For a given CAC score, high CAC density relative to plaque area confers lower long-term ASCVD risk, likely serving as an imaging marker of biological resilience for lesion stability.
The main clinical implication of our findings relates to the concept of risk refinement among persons with prevalent CAC, which may ultimately guide more precision-based preventive pharmacotherapies according to calcium density and area groups. Our study consisted almost entirely of participants of Caucasian ethnicity and a low proportion of women were included, therefore future studies in more diverse samples are required to understand the relationship between calcium area-density discordance on ASCVD risk.
References
- Arnett DK, Blumenthal RS, Albert MA, et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2019;74:e177–e232.
- Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2021;42:3227-337.
- Blaha MJ, Mortensen MB, Kianoush S, Tota-Maharaj R, Cainzos-Achirica M. Coronary artery calcium scoring: is it time for a change in methodology? JACC Cardiovasc Imaging 2017;10:923-37.
- Razavi AC, Agatston AS, Shaw LJ, et al. Evolving role of calcium density in coronary artery calcium scoring and atherosclerotic cardiovascular disease risk. JACC Cardiovasc Imaging 2022;15:1648–62.
Clinical Topics: Congenital Heart Disease and Pediatric Cardiology, Prevention, Atherosclerotic Disease (CAD/PAD), Congenital Heart Disease, CHD and Pediatrics and Arrhythmias, CHD and Pediatrics and Prevention, CHD and Pediatrics and Quality Improvement, Noninvasive Imaging
Keywords: Coronary Artery Disease, Plaque, Atherosclerotic, Calcium, Body Mass Index, Cardiovascular Diseases, Prevalence, Follow-Up Studies, Blood Pressure, American Heart Association, Risk Assessment, Risk Factors, Primary Prevention, Diabetes Mellitus, Heart Defects, Congenital, Risk Reduction Behavior, Algorithms, Phenotype
< Back to Listings