

ACC Expert Consensus Decision Pathway Focuses on Evaluation and Disposition of Acute Chest Pain in the ED
ACC's newest Expert Consensus Decision Pathway aims to provide structure around the rapid "evaluation and disposition of acute chest pain" in patients presenting to the emergency department (ED) for possible acute coronary syndrome. The document, published Oct. 11 in JACC, also encourages the use of rapid clinical decision pathways alongside high-sensitivity cardiac troponin I (hs-cTnI) assays that may help hospitals solve for some of the ED challenges.
"At the institution level, this Expert Consensus Decision Pathway recommends implementation of hs-cTn assays in conjunction with a clinical decision pathway to reduce ED 'dwell' times and increase the proportion of patients with chest pain who can safely be discharged without additional testing," write Writing Committee Chair Michael C. Kontos, MD, FACC, and Vice Chair James A. de Lemos, MD, FACC, et al. "Successful implementation will decrease ED crowding and limit unnecessary testing."
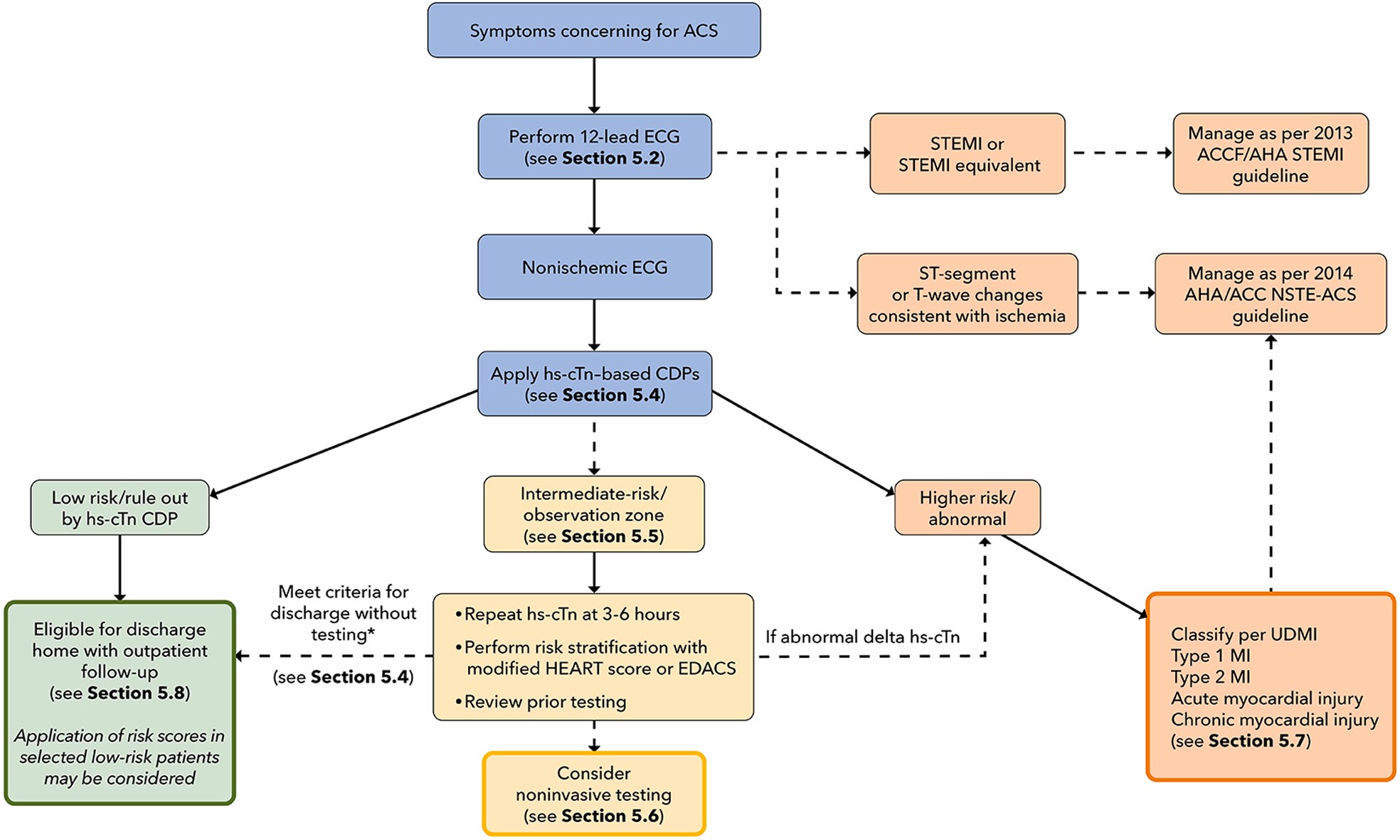
The Pathway also urges a strategic focus at the patient level on "accelerating the evaluation process and matching the intensity of testing and treatment to patient risk." Engagement of a multidisciplinary team that includes emergency medicine, laboratory medicine, cardiology, and hospital medicine specialties, along with careful ECG review, the inclusion of appropriate patients into a clinical decision pathway that "combines hs-cTn measurements with risk assessment, and selective use of noninvasive testing" are key to this process.
"The ECG remains the best initial test for chest pain evaluation because it is rapid, inexpensive and provides critical diagnostic and prognostic information," say Kontos and de Lemos. They note that institutions should work to transition to hs-cTn assays given that their increased sensitivity and precision offer substantial advantages for the accelerated "rule out" of myocardial infarction and can eliminate the need for noninvasive testing in most low-risk patients.
Both Kontos and de Lemos, as well as the broader Writing Committee, stress that the clinical decision pathway should augment – not replace – triage, treatment and disposition decisions and that a "provider's clinical judgment at the bedside remains an indispensable tool that may lead to different triage decisions than those suggested by the clinical decision pathway."
For patients who are determined to be at intermediate risk, additional observation and/or additional noninvasive testing may be required. Patient factors, such as results of prior testing, availability of tests, timeliness of test reporting and institutional expertise should be considered when determining choice of noninvasive tests.
Access the full Expert Consensus Decision Pathway.
Clinical Topics: Acute Coronary Syndromes, Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Stable Ischemic Heart Disease, Vascular Medicine, Statins, Acute Heart Failure, Interventions and ACS, Interventions and Imaging, Interventions and Vascular Medicine, Computed Tomography, Nuclear Imaging, Chronic Angina
Keywords: Chest Pain, Emergency Service, Hospital, Troponin I, Troponin T, ST Elevation Myocardial Infarction, Acute Coronary Syndrome, Angina, Stable, Computed Tomography Angiography, Patient Care Team, Patient Care, Emergency Medicine, Heart Failure, Hemodynamics, Cytidine Diphosphate
< Back to Listings