A 78-year-old Caucasian man presents with a history of atrial fibrillation on anticoagulation with an oral direct antithrombin inhibitor, heart failure with preserved ejection fraction (HFpEF) of 50% hypertension, dyslipidemia, and obesity (BMI = 32 kg/m2).
He was hospitalized two weeks ago due to heart failure exacerbation. He was treated with intravenous diuresis that improved his hypoxemia, dyspnea, and peripheral edema; however, respiratory assessment during hospitalization showed an asymptomatic on-and-off tachypnea (Figure 1). He was discharged on optimal medical therapy as per guidelines including metoprolol, dabigatran, lisinopril, atorvastatin, furosemide, spironolactone, digoxin, and insulin subcutaneous with plan for follow-up as an outpatient.
Figure 1
(Click to Enlarge)
Last week, he was evaluated by his primary physician at the outpatient clinic. He reported no signs of heart failure decompensation. He complained of daytime fatigue and nonrestorative sleep. His primary physician recommended an overnight oximetry, which was completed two nights ago (Figure 2). Unfortunately, today he developed acute shortness of breath that leads him to the emergency department.
Figure 2
(Click to Enlarge)
This hospitalization represents the third one in the last six months. He reports dyspnea at rest and worsening bilateral lower extremity edema. His vital signs are heart rate of 115 beats per minute, irregularly irregular pulse, respiratory rate of 24 breaths per minutes, blood pressure of 105/76 mm Hg, and oxyhemoglobin saturation of 85% at room air.
Which of the following statements is TRUE regarding sleep apnea in heart failure?
Show Answer
The correct answer is: C. Untreated sleep-disordered breathing has been associated with a higher number of readmissions.
This patient's overnight oximetry is suggestive of sleep-disordered breathing with multiple continued oscillatory desaturation events (284 events per 4.5 hours = 63 events per hours of oxygen desaturation greater than 4%; normal range is less than five events per hours). Considering the minimal oxygen desaturation related to a high oxygen desaturation index (ODI) (above 30 events per hour), it is likely this patient has developed Cheyne-Stokes respiration with central sleep apnea (CSR-CSA). This specific pattern on the overnight oximetry is highly suggestive of central sleep apnea with a reported sensitivity as high as 83% in heart failure patients and close to 100% in patients with atrial fibrillation, although its specificity is less than ideal (close to 20%).1
CSR-CSA is characterized by a cyclic breathing pattern that alternates episode of apnea followed by a crescendo-decrescendo tachypnea/hypernea.2 It is believed that ventilatory control dysregulation due to an exaggerated response to CO2 plus prolonged brain-lung circulation time is the underlying cause of CSR. Sleep-disordered breathing is highly prevalent in heart failure patients.3,4 and central sleep apnea can represent close to half of those cases.5 Central sleep apnea in HF patients has been associated with poor outcomes6,7 in some, but not all, studies.
The first treatment of CSR-CSA in the setting of HF is optimization of pharmacotherapy. Persistent disordered breathing with symptoms might warrant positive airway pressure therapy. As opposed to its efficacy in obstructive sleep apnea (OSA), continuous positive airway pressure (CPAP)8 is typically effective in a minority of patients with CSR-CSA. Adaptive servo ventilation (ASV), on the other hand, has been associated with better control of CSR-CSA and improved treatment compliance,9 though the results of multicenter trials are awaited. Treatment of Predominant Central Sleep Apnoea by Adaptive Servo Ventilation in Patients With Heart Failure (Serve-HF) and Effect of Adaptive Servo Ventilation (ASV) on Survival and Hospital Admissions in Heart Failure (ADVENT-HF) are large prospective randomized controlled trails that are evaluating the magnitude of the effect of treatment with ASV in heart failure patients.
Recently, Khay at et al. evaluated the impact of central sleep apnea as a predictor of cardiac readmission in hospitalized patients. This prospective study followed, for up to six months, 165 patients with CSA from a cohort of 784 heart failure patients. After adjustment of cofounding variables, it was concluded than CSA represented an increased risk for hospital readmission with an odds ratio of 1.53 (95% confidence interval [CI] 1.1-2.2; p = 0.03) when compared with heart failure without sleep-disordered breathing.10 Furthermore, there was a suggestion of increased mortality associated with sleep-disordered breathing with follow-up for up to three years.11
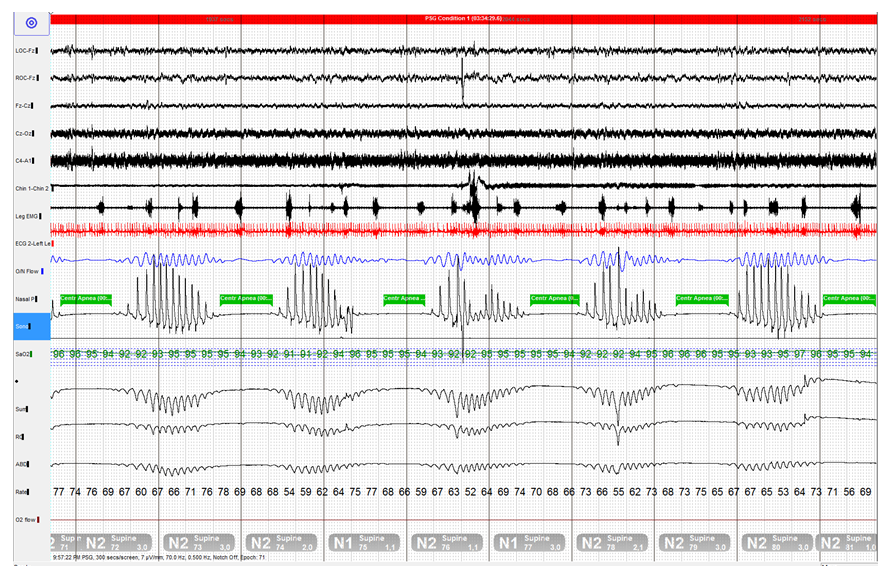
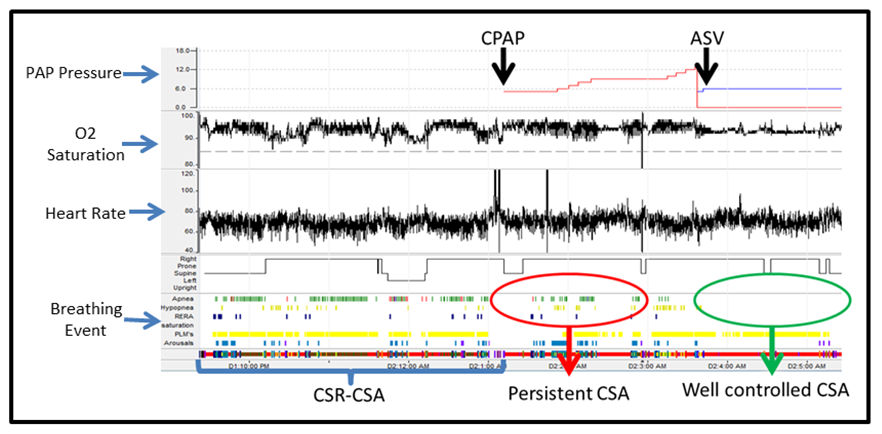
In this patient, a split-night polysomnography study confirmed the diagnosis of CSR-CSA (Figure 3). CPAP was ineffective to control his sleep-disordered breathing and ASV showed complete control of central sleep apnea (Figure 4). Therefore, the patient was prescribed ASV.
Figure 3
(Click to Enlarge)
Polysomnography is showing 5 minutes of monitoring sleep. The green box highlighted the central apnea events that cycle with crescendo-decrescendo breathing pattern evidence by larger respiratory efforts.
Figure 4
(Click to Enlarge)
This figure demostrates the changes of heart rate and oxygen saturation and breathing events (apneas and hypopneas) during overnight sleep study. The first segment of the night patient's breathing was unsupported, and there were multiple breathing events. After CPAP therapy, breathing improved oxygenation, but breathing events remained persistent. On the third segment, it is evident that ASV was able to control breathing events with normalization of oxygen saturation.
Nocturnal oxygen therapy along with optimal medical therapy for heart failure showed improvement in patients' quality of life (QOL), and left ventricular function. However, there were no changes in clinical outcome when compared with a control group receiving heart failure standard therapy alone.12,13 When compared to positive airway pressure, nocturnal oxygen was inferior as a means to improve the apnea hypopnea index.14 Current practice guidelines recommend nocturnal oxygen therapy for those patients with central sleep apnea related to chronic heart failure who are unable to comply with CPAP therapy15 and not as an initial therapeutic option, rendering answer option A the wrong answer.
Mandibular advance devices treat obstructive sleep apnea by traction on the jaw to increase upper airway luminal size by several millimeters. Such an effect wouldn't impact central sleep apnea, which occurs independently of upper airway caliber.
Finally, head elevation has been used as a temporary measure in the postsurgical care of OSA patients.16 The rationale of this approach is based on the attenuation of gravity effect on soft tissues that obstruct the airway. It's unlikely that such an intervention would impact this patient's condition.
References
Series F, Kimoff RJ, Morrison D, et al. Prospective evaluation of nocturnal oximetry for detection of sleep-related breathing disturbances in patients with chronic heart failure. CHEST 2005;127:1507-14.
Cherniack NS, Longobardo GS. Cheyne-Stokes breathing. An instability in physiologic control. N Engl J Med 1973;288:952-7.
Khayat RN, Jarjoura D, Patt B, Yamokoski T, Abraham WT. In-hospital testing for sleep-disordered breathing in hospitalized patients with decompensated heart failure: report of prevalence and patient characteristics. J Cardiac Fail 2009;15:739-46.
Paulino A, Damy T, Margarit L, et al. Prevalence of sleep-disordered breathing in a 316-patient French cohort of stable congestive heart failure. Arch Cardiovasc Dis 2009;102:169-75.
Sin DD, Fitzgerald F, Parker JD, Newton G, Floras JS, Bradley TD. Risk factors for central and obstructive sleep apnea in 450 men and women with congestive heart failure. Am J Respir Crit Care Med 1999;160:1101-6.
Javaheri S, Shukla R, Zeigler H, Wexler L. Central sleep apnea, right ventricular dysfunction, and low diastolic blood pressure are predictors of mortality in systolic heart failure. J Am Coll Cardiol 2007;49:2028-34.
Lanfranchi PA, Braghiroli A, Bosimini E, Mazzuero G, Colombo R, Donner CF, Giannuzzi P. Prognostic value of nocturnal Cheyne-Stokes respiration in chronic heart failure. Circulation 1999;99:1435-40.
Buckle P, Millar T, Kryger M. The effect of short-term nasal CPAP on Cheyne-Stokes respiration in congestive heart failure. CHEST 1992;102:31-5.
Philippe C, Stoica-Herman M, Drouot X, et al. Compliance with and effectiveness of adaptive servoventilation versus continuous positive airway pressure in the treatment of Cheyne-Stokes respiration in heart failure over a six month period. Heart 2006;92:337-42.
Khayat R, Abraham W, Patt B, et al. Central sleep apnea is a predictor of cardiac readmission in hospitalized patients with systolic heart failure. J Cardiac Fail 2012;18:534-40.
Khayat R, Jarjoura D, Porter K, et al. Sleep disordered breathing and post-discharge mortality in patients with acute heart failure. Eur Heart J 2015:ehu522.
Sasayama S, Izumi T, Matsuzaki M, Matsumori A, Asanoi H, Momomura S-i, Seino Y, Ueshima K. Improvement of quality of life with nocturnal oxygen therapy in heart failure patients with central sleep apnea. Circulation 2009;73:1255-62.
Nakao YM, Ueshima K, Yasuno S, Sasayama S. Effects of nocturnal oxygen therapy in patients with chronic heart failure and central sleep apnea: CHF-HOT study. Heart Vessels 2014 Oct 8. [Epub ahead of print]
Teschler H, Döhring J, Wang Y-M, Berthon-Jones M. Adaptive pressure support servo-ventilation: a novel treatment for Cheyne-Stokes respiration in heart failure. Am J Respir Crit Care Med 2001;164:614-9.
Aurora RN, Chowdhuri S, Ramar K, et al. The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analyses. Sleep 2012;35:17-40.
Mickelson SA. Preoperative and postoperative management of obstructive sleep apnea patients. Otolaryngol Clin North Am 2007;40:877-89.