A 29-year-old man with double outlet right ventricle, transposition of the great arteries, ventricular septal defect, and pulmonary stenosis was treated with the Rastelli procedure as an infant. He underwent right ventricle (RV) to pulmonary artery (PA) conduit replacement in his teenage years and successfully underwent Melody transpulmonary valve (Medtronic, Inc., Minneapolis, MN) implantation 3 months prior to presentation due to conduit stenosis with a gradient of 70 mm Hg in the presence of New York Heart Association Class III symptoms. The patient presented (3 months post-surgery) with near syncope and significant chest pain while exercising on his treadmill at home. He was diaphoretic, felt unwell, and presented to the emergency department with hypotension and wide complex tachycardia at a rate of 200 bpm. The emergency department physician cardioverted the patient electrically into sinus rhythm. A physical exam revealed displaced apex and a precordial heave. He had rales bilaterally, a single S2, and an S3. His pertinent laboratory findings included troponin of I7.8 ng/ml and creatine kinase of 530 units/L. A post-cardioversion electrocardiogram showed q waves inferiorly but no evidence of ST-segment elevation myocardial infarction (MI).
What was the most likely missed step in work-up of this patient prior to transpulmonary valve implantation?
Show Answer
The correct answer is: B. Balloon inflation in right ventricular outflow tract (RVOT) and simultaneous coronary artery angiography
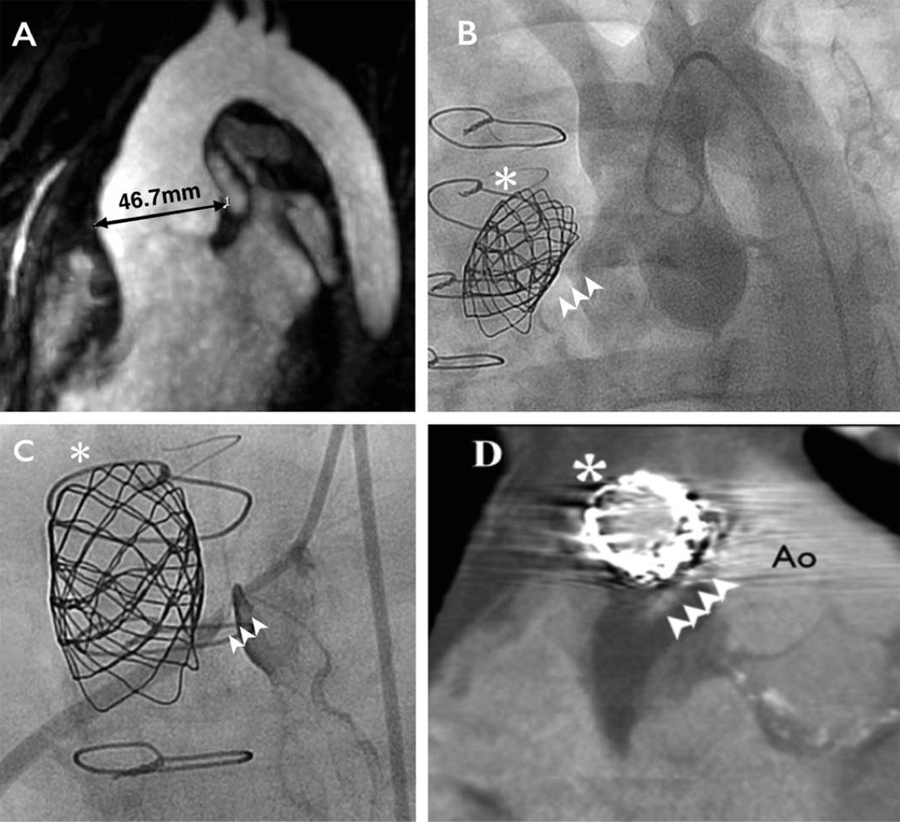
Coronary artery disease is not uncommon in adults with congenital heart disease. Although atherosclerotic disease should be suspected in members of this population as they enter their fourth decade of life, other mechanisms should also be suspected. Examples include anatomic obstruction due to coronary translocation during previous cardiac surgeries, abnormal sheer stress placed upon the coronary endothelium due to altered flow, associated anomalous coronary arteries, and abnormal relationship between the RVOT, coronary arteries, and dilated aorta. In reviewing this case, pre-operative cardiac magnetic resonance imaging confirmed a dilated aorta at 4.7 cm (Figure 1A). Because no coronary anomalies were seen, the patient missed the required step of simulation testing with balloon inflation in RVOT and simultaneous coronary artery angiography. After he presented with MI, an aortogram (Figure 1B) confirmed proximity of the dilated sinuses and right coronary artery (RCA) ostium (see multiple arrow heads in figures). Dissection of RCA ostium was suggested during angiography (Figure 1C) and then confirmed with cardiac computed tomography (Figure 1D). The most likely mechanism of infarction in the patient can be ascribed to a combination of two mechanisms. First, the increase in cardiac output during exercise leads to further aortic dilatation and therefore compresses the RCA ostium against the RV to PA conduit that was recently dilated during transpulmonary valve implantation. This aorta-conduit relationship had been distorted at the time of stented valve implantation and likely further compromised due to torque, tension, and/or stent fracture. Second, exercise-mediated increased demand unmasked a fixed coronary supply given the trauma that may have occurred to the RCA ostium. A key take-home message is that every adult patient with congenital heart disease who has had an intervention close to a coronary artery, particularly in relation to a rigid structure (such as a Melody transpulmonary valve [Medtronic Inc., Minneapolis, MN]), is at risk of torque, tension, and/or compression. Therefore, coronary patency and ischemia must be considered even late after intervention. Answer A is incorrect because diagnostic angiography alone does not show the relationship of RVOT to the coronary arteries. Answer C is incorrect because anatomic visualization is necessary, not functional testing. And answer D is incorrect because the wide complex tachycardia on presentation that was a sign of the patient's MI is an arrhythmia that would have not been picked up by electrophysiology study.
Figure 1
References
McElhinney DB, Hellenbrand WE, Zahn EM, et al. Short- and medium-term outcomes after transcatheter pulmonary valve placement in the expanded multicenter US melody valve trial. Circulation 2010;122:507-16.
Dehghani P, Kraushaar G, Taylor D. Coronary artery compression three months after transcatheter pulmonary valve implantation. Catheter Cardiovasc Interv 2015;85:611-4.