An 82-year-old female patient with a history of calcific aortic stenosis (AS), hypertension treated with angiotensin-converting enzyme inhibitors, and renal failure with creatinine at 2 mg/dl presented with New York Heart Association Class III dyspnea and was recently hospitalized for heart failure. She was treated successfully with diuretics. Her blood pressure at admission was 135/65 mmHg with a body surface area of 1.8 m2, and her heart rate was 90 bpm. The electrocardiogram showed sinus rhythm; there was no evidence of acute ischemic changes. The Doppler-echocardiogram performed during this hospitalization revealed the following:
Left ventricular ejection fraction (LVEF) at 75% (Video 1)
Left ventricular (LV) end-diastolic diameter = 41 mm
Left ventricular outflow tract (LVOT) diameter = 21 mm
Left atrial volume index = 35 ml/m2
Grade II LV diastolic dysfunction
Parasternal long and short axis views (Videos 2-3) showed thickened and calcified aortic valve (AV) leaflets with reduced opening. There was only mild mitral regurgitation. Stroke volume measured by Doppler method in the LVOT was 59 mL (Figure 1, top). Transvalvular aortic mean gradient was 31 mmHg after multi-window interrogation with continuous wave Doppler, and peak velocity was 3.6 m/s (Figure 1, bottom). Aortic valve area (AVA) by continuity equation was 0.84 cm2, indexed AVA was 0.47 cm2/m2, and Doppler-velocity index was 0.24 (Figure 1). There were no other notable abnormalities.
Figure 1
Video 1
Video 2
Video 3
Which of the following is the best next step in management?
Show Answer
The correct answer is: E. Further investigation to confirm AS severity. Perform dobutamine stress echocardiography or valve calcium scoring.
Low gradient AS is defined as an AVA <1cm2 and mean gradient <40 mmHg, and there are different patterns of low-gradient AS. The classic low-flow, low-gradient AS, which is the form of low-gradient AS that is associated with reduced ejection fraction, is called D2 stage in the guidelines. The paradoxical low-flow, low-gradient AS (D3 stage) is characterized by low-
flow state (SVi < 35 mL/m2) despite preserved LVEF (>50%). The low flow is mainly due to pronounced LV concentric remodeling with a small LV cavity size, diastolic dysfunction, and reduced longitudinal shortening.1 The third type of low gradient AS is characterized by normal flow and is not addressed in the guidelines.2
At rest echocardiography, this patient had an AVA and Doppler velocity index in the severe range, and mean gradient and maximum aortic flow velocity was in the moderate range. Thus, the severity of AS was uncertain, and further investigation was required. The patient had a low flow (stroke volume indexed to a body surface area of 32 mL/m2, which is <35ml/m2 and the cut-off for low flow) with a preserved LVEF. This was thus a case of paradoxical low-flow, low-gradient AS, and the next step is to differentiate between a true stenosis and a pseudo-severe stenosis.
To assess the severity of the AS, one may consider performing a test to increase or ideally normalize transvalvular flow rate. However, given the symptomatic status of the patient, the exercise stress echocardiography is contra-indicated; therefore, answer D is incorrect. Dobutamine stress echocardiography could be used; therefore, answer E is the best option.3 However, dobutamine stress in patients with normal ejection fraction, concentric hypertrophy, and diastolic dysfunction may not be able to increase flow rate and may be associated with side effects.4 Hence, AV calcification quantitation by computed tomography (CT) may be the best option to confirm AS severity in this patient. Recent studies have shown that calcium score >1200 in women and >2000 in men was accurate to identify severe AS.5 One could argue that assessment of the morphology of the AV at echocardiography (severely thickened and calcified valve) was consistent with severe AS, and thus no more investigation was necessary, and patient could have been sent to AV replacement just based on echocardiography. Nevertheless, echocardiographic assessment of AV calcification is only semi-quantitative and correlates weakly with AV calcification score by CT.6 In addition, symptoms may be related do diastolic heart failure but not to the AS that could be only moderate. Thus, assessing the true severity of AS should be done with a robust method (dobutamine stress echocardiography or CT) before making a crucial clinical decision regarding AV replacement. Therefore, answers A-C are not the best options.
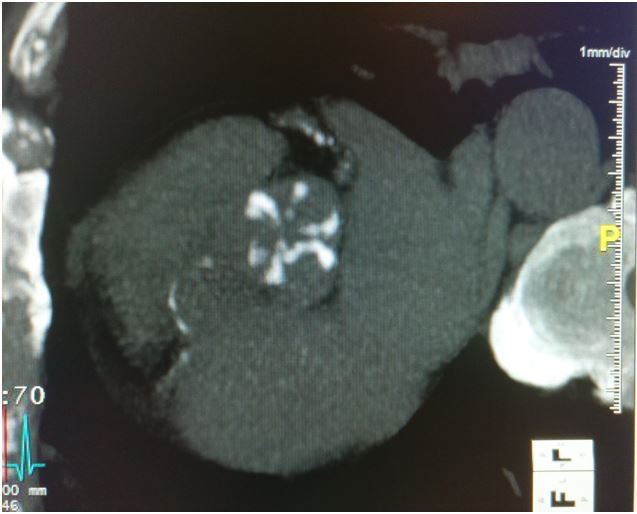
Our patient underwent a CT scan and computed tomography calcium score was 1310 AU (Figure 2), which is consistent with severe AS. Given that the patient had a Society of Thoracic Surgeons score of 8.3% with a small aortic annulus (high risk of severe prosthesis-patient mismatch7), the heart team decided to perform a transfemoral transcatheter AV replacement with a 23 mm Edwards SAPIEN-3 valve (Edwards Lifesciences; Irvine, CA). Post-procedure Doppler echocardiography showed a good result with mean gradient of 12 mmHg, AVA of 1.4 cm2, and no paravalvular leak.
According to American and European guidelines,8,9 there is a Class IIa recommendation for AV replacement in symptomatic normotensive patients after confirmation of AS severity. However, the guidelines do not recommend a specific algorithm to be followed in the assessment of AS severity. There are several ways to confirm AS severity, including assessment of AV morphology by transthoracic or transesophageal echocardiography, dobutamine stress echocardiography, or AV calcium scoring by CT. In this patient with paradoxical low-flow, low-gradient AS, the most appropriate approach was probably to use AV calcium scoring to confirm AS severity.
Figure 2
References
Pibarot P, Dumesnil JG. Low-flow, low-gradient aortic stenosis with normal and depressed left ventricular ejection fraction. J Am Coll Cardiol 2012;60:1845-53.
Clavel MA, Burwash IG, Pibarot P. Cardiac Imaging for Assessing Low-Gradient Severe Aortic Stenosis JACC Cardiovasc Imaging 2017;10:185-202.
Clavel MA, Ennezat PV, Maréchaux S, et al. Utility of stress echocardiography to confirm stenosis severity and predict outcome in patients with low flow, low gradient aortic stenosis and preserved lv ejection fraction. Canadian J Cardiol 2011;27:S25-2.
Lancellotti P, Pellikka PA, Budts W, et al. The clinical use of stress echocardiography in non-ischaemic heart disease: recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur Heart J Cardiovasc Imaging 2016;17:1191-229.
Clavel MA, Messika-Zeitoun D, Pibarot P, et al. The complex nature of discordant severe calcified aortic valve disease grading: new insights from combined Doppler echocardiographic and computed tomographic study. J Am Coll Cardiol 2013;62:2329-38.
Messika-Zeitoun D, Aubry MC, Detaint D, et al. Evaluation and clinical implications of aortic valve calcification measured by electron-beam computed tomography. Circulation 2004;110:356-62.
Dahou A, Mahjoub H, Pibarot P. Prosthesis-Patient Mismatch After Aortic Valve Replacement. Curr Treat Options Cardiovasc Med 2016;18:67.
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2014;63:e57-185.
Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC), European Association for Cardio-Thoracic Surgery (EACTS), Vahanian A, et al. Guidelines on the management of valvular heart disease (version 2012). Eur Heart J 2012;33:2451-96.