A 60-year-old male patient with a prior history of diabetes mellitus type II, hypertension, and mitral valve replacement with mechanical prosthesis in 2012 on warfarin presented to the hospital with lethargy, nausea, vomiting, and intermittent fevers for 2 weeks. The patient was appropriately treated for a urinary tract infection with 2 rounds of antibiotics in the last 2 weeks prior to presentation. The patient also complained of mild blurriness of vision in both eyes. His blood pressure was 110/70 mmHg, and his heart rate was 48 bpm with normal oxygen saturation at room air. He was febrile to 102°C and was oriented to person, place, and time but exhibited minimal confusion. His exam was significant for a mechanical click on cardiac auscultation. The patient did not exhibit any significant abnormalities on physical examination, and there was no evidence of focal deficits. Figure 1 shows his electrocardiogram at presentation. Computed tomography (CT) scan of the brain was suspicious for a very small right subarachnoid hemorrhage. His international normalized ratio (INR) level was elevated at 9 on laboratory testing.
Figure 1
The electrocardiogram demonstrated atrioventricular (AV) dissociation and complete heart block.
Which of the following is the next best step in management?
Show Answer
The correct answer is: D. Get blood cultures, start empiric intravenous antibiotics, schedule patient for magnetic resonance imaging (MRI) of the brain and transesophageal echocardiogram (TEE).
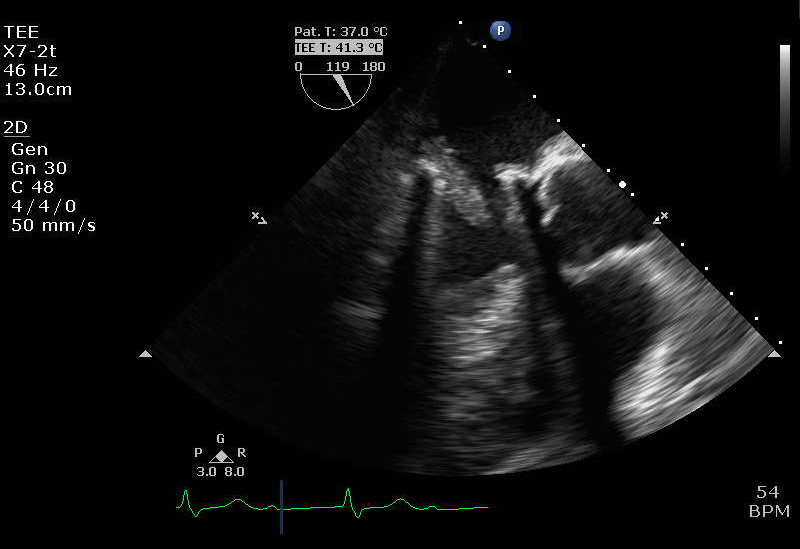
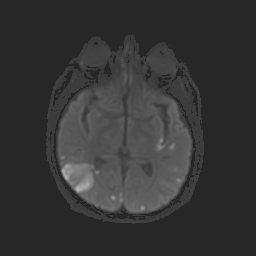
The patient was started on empiric antibiotics after acquiring blood cultures. A TEE revealed multiple vegetations attached to the mechanical mitral valve and annulus, the largest one being 2.5 x 1.2 cm with thickening of the intervalvular fibrosa and a high probability of underlying abscess (Videos 1-2 and Figure 2). MRI of the brain was obtained (Figure 3), which revealed multiple sites of cerebral infarction concerning for emboli but with no evidence of bleeding. Blood cultures were positive for a sensitive strain of enterococcus fecalis. The patient was taken for a redo sternotomy with repeat mitral valve replacement and debridement of the mitral annular abscess with placement of a bovine pericardial annular patch to prevent a residual atrial septal defect. The procedure was performed successfully without complication. A repeat CT scan of the head showed no evidence of bleeding. The patient subsequently received a transvenous permanent pacemaker for persistence of complete heart block. He was discharged on a prolonged intravenous antibiotic course consisting of ampicillin and ceftriaxone.
Video 1: TEE Showing Prosthetic Mitral Valve Endocarditis
Video 2: TEE Showing Prosthetic Mitral Valve Endocarditis
Figure 2
TEE shows presence of mechanical mitral valve and the presence of more than one vegetation attached to the mitral valve and annulus with thickening of the intervalvular fibrosa.
Figure 3
MRI of the brain shows multiple areas of acute infarction in more than one vascular territory.
Patients with a prosthetic valve are at increased risk for infective endocarditis (IE), invasion of the perivalvular apparatus with formation of abscess or fistula and embolic events in addition to significant prosthetic valvular dysfunction. Patients with prosthetic valve endocarditis (PVE) commonly experience clinically significant arterial embolism, with evidence of central nervous system complications (embolism and/or hemorrhages) in 20-40% of the cases. High-degree AV conduction block and bundle branch block has been seen with development of perivalvular abscess and progression of infection into the bundles or the AV node.1,2 Graupner et al. showed that the presence of AV block was 97% specific in detecting involvement of the aortic perivalvular region.1
The 2015 American Heart Association scientific statement on IE recommends early surgery in patients with persistent vegetations after systemic embolization, anterior mitral valve leaflet >10 mm, ≥1 embolic events or increased vegetation size despite treatment, severe valvular dysfunction such as acute aortic or mitral insufficiency with signs of ventricular failure, persistent heart failure, valve perforation or rupture, perivalvular extension, fistula formation, new heart block, and development of a large abscess and progression despite treatment.3
Factors associated with increased in-hospital and 1-year mortality in patients with PVE are older age, healthcare-associated infection, S.aureus infection, persistent bacteremia, heart failure, intracardiac abscess, valve dehiscence, and stroke.4 Projected mortality of patients with paravalvular infection is expected to be 100% in the absence of surgical intervention, and prior studies have shown operative mortality rates of 10-30% with experienced cardiac surgeons.5 Thus, early surgery may be lifesaving in patients with PVE and extension of disease into the paravalvular apparatus.
Use of vitamin K in patients with mechanical prosthetic valves is advised with caution due to its potential for lowering INR and increasing potential for valve thrombosis and related complications. In this case, where bacterial prosthetic endocarditis was likely based on presentation, looking at viral etiology, initiating transcutaneous or transvenous pacing and intravenous isoprenaline may have potential benefit in select clinical situations but do not represent the next best step in management here.
References
Graupner C, Vilacosta I, SanRomán J, et al. Periannular extension of infective endocarditis. J Am Coll Cardiol 2002;39:1204-11.
Bacchion F, Cukon S, Rizzoli G, et al. Infective endocarditis in bicuspid aortic valve: atrioventricular block as sign of perivalvular abscess. Cardiovasc Pathol 2007;16:252-5.
Baddour LM, Wilson WR, Bayer AS, et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015;132:1435-86.
Lalani T, Chu VH, Park LP, et al. In-hospital and 1-year mortality in patients undergoing early surgery for prosthetic valve endocarditis. JAMA Intern Med 2013;173:1495-504.
Hill EE, Herregods MC, Vanderschueren S, Claus P, Peetermans WE, Herijgers P. Management of prosthetic valve infective endocarditis. Am J Cardiol 2008;101:1174-8.