Ten Points to Remember From the Recent AHA Scientific Statement on "Cardiovascular Toxicity in Patients Treated for Childhood Cancer"
Quick Takes
- There are approximately 500,000 survivors of pediatric cancer in the United States, and many key therapies put those individuals at risk of cardiovascular disease (CVD) during their lifetimes.
- The risk of CVD is well described for anthracyclines and radiotherapy; many novel therapies (e.g., small molecule inhibitors, antibody conjugates, immunotherapies) also carry risk, although the ability to predict their risks is not as refined as for traditional therapies.
- CVD in survivors of childhood cancer is more than just ventricular dysfunction, and includes metabolic effects, hypertension, arrhythmia, and thrombosis; understanding an individual's risk and establishing appropriate screening is a key component to patient care.
Pediatric cardio-oncology has expanded in scope over the past several decades to address the ever-increasing issues related to cardiovascular disease (CVD) in patients with and survivors of cancer, related both to treatment modalities and the disease itself. It is increasingly recognized that all cancer treatments can pose short- or long-term risks of developing CVD, made more impactful by potential long lifespans afterward. Anthracycline chemotherapy and chest-directed radiotherapy are the archetypal cardiotoxic therapies, and modern approaches have contributed to improved cardiovascular (CV) outcomes for survivors through dose reduction, organ blocking, and concomitant cardioprotective therapies. However, whereas novel treatments—such as small molecule inhibitors, antibody-based cytotoxic therapy, and immunotherapy—have expanded options for cancers that were previously difficult to treat, they also uncover new cardiotoxic risks. Structured and effective surveillance strategies along with prevention and treatment of extant CVD are of utmost importance. Accordingly, the 2025 American Heart Association (AHA) scientific statement on CV Toxicity in Patients Treated for Childhood Cancer was developed.1
What follows are 10 key points from the statement:
- Pediatric cancer prevalence. Children account for approximately 5% of all new cancer diagnoses in the United States. Coupled with 5-year survival rates of >85% overall, there are nearly 500,000 survivors of pediatric cancer. Given the potential for decades of survival after treatment, there is an aging population at risk of cancer treatment–related CVD.
- Risk of developing CVD in survivors of childhood cancer. Treatments well known to contribute to CVD in survivors of childhood cancer include anthracycline chemotherapy, radiotherapy, alkylators, and platinum agents (Figure 1). Validated risk calculators are available through the CCSS (Childhood Cancer Survivor Study) to predict the risk of heart failure (HF), ischemic heart disease, and stroke. Newer therapies (discussed later) are known to have association with CVD but precise risk prediction is not available. Although there are strategies to limit cardiotoxicity for anthracyclines and radiotherapy, no such mitigation has yet been identified for most novel therapies.
Figure 1: Pharmacological and Nonpharmacological Cancer Therapies With Reported Effects on the CV System in Pediatric Patients
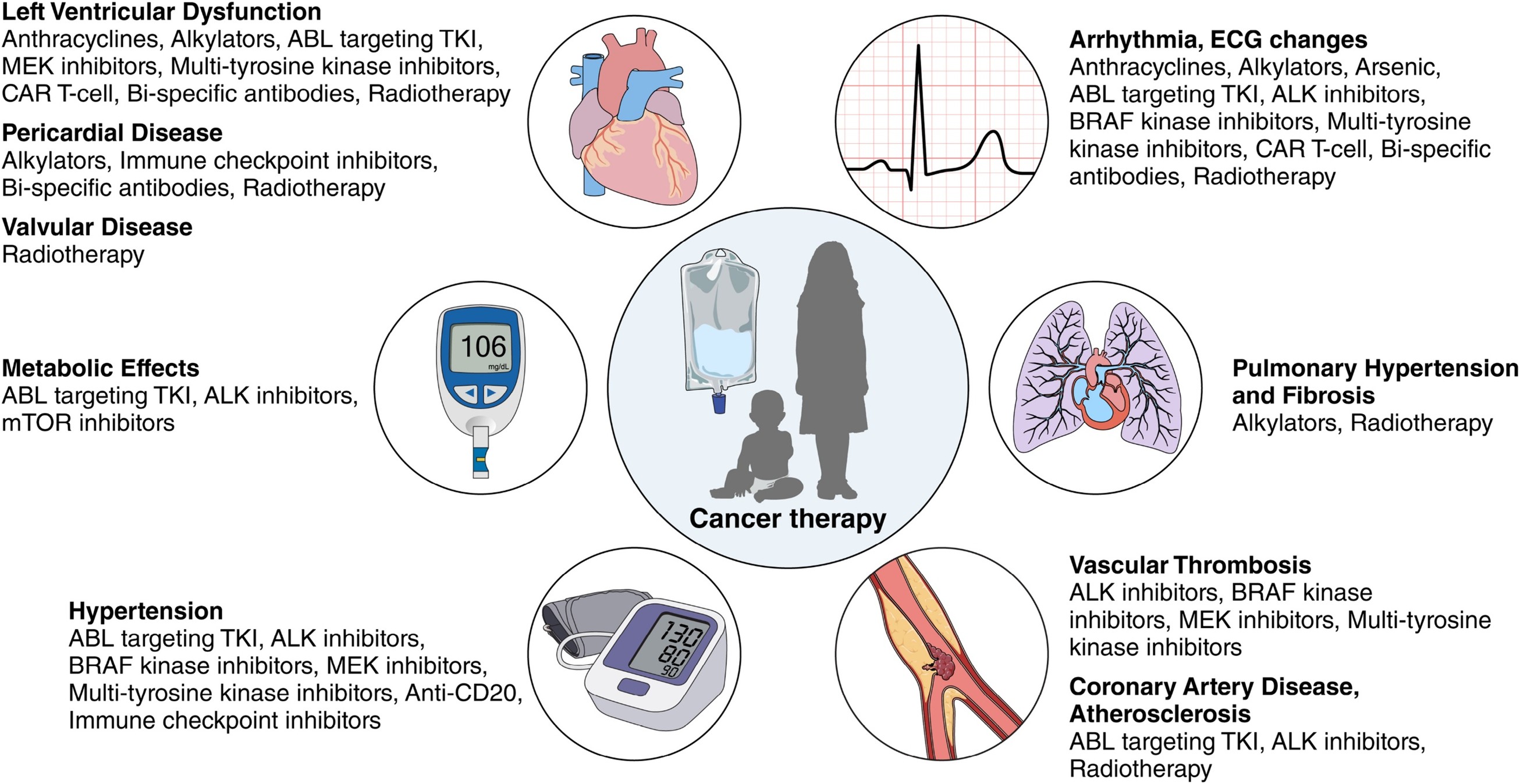
Reprinted with permission. Circulation.2025;151:e926-e943. ©2025 American Heart Association, Inc.
ABL = ABL proto-oncogene; ALK = anaplastic lymphoma kinase; BRAF = B-Raf proto-oncogene, serine/threonine kinase; CAR = chimeric antigen receptor; CV = cardiovascular; ECG = electrocardiogram; MEK = mitogen-activated protein kinase; mTOR = mammalian target of rapamycin; TKI = tyrosine kinase inhibitor.
- Novel therapies: small molecule inhibitors. These agents include kinase and nonkinase inhibitors, and they have a role in treating leukemias, lymphomas, and some solid cancers. CV effects occur primarily in the form of arrhythmia or electrocardiogram (ECG) changes, hypertension (HTN), and thrombosis. Left ventricular (LV) dysfunction is seen more often in kinase inhibitors than in nonkinase inhibitors and is generally reversible with discontinuation of the agent (Figure 1).
- Novel therapies: antibody conjugates. These therapies include monoclonal antibodies used for several liquid and solid cancers. LV dysfunction, HTN, and arrhythmia and ECG changes are most common.
- Novel therapies: immunotherapies. New immunotherapies offer a new avenue to treat leukemias, lymphomas, and, particularly, solid cancers. The immune checkpoint inhibitors, which target apoptosis pathways, are associated with arrhythmia and, rarely, fatal myocarditis. For chimeric antigen receptor T-cell therapies, cardiotoxicity (e.g., cardiomyopathy, arrhythmia, hypotension/shock, and cardiac arrest) can occur in up to one-third of pediatric, young adult, and adult patients, primarily associated with cytokine release syndrome (Figure 1). Treatment with interleukin-6 inhibition may counteract this effect.
- Surveillance. Early recognition of CVD is important to maximize the impact of treatment (Figure 2). The American Society of Echocardiography (ASE) released updated recommendations for echocardiographic surveillance including use of two-dimensional, three-dimensional, and strain imaging.2 Cardiac magnetic resonance imaging has a role when echocardiography is limited, and recently has been used to more accurately predict patients at increased risk. Plasma biomarkers may be of use in pediatric patients but are not as well established as they are for adult cohorts.
Figure 2: Care of the Patient With Pediatric CTRC Through the Age Spectrum
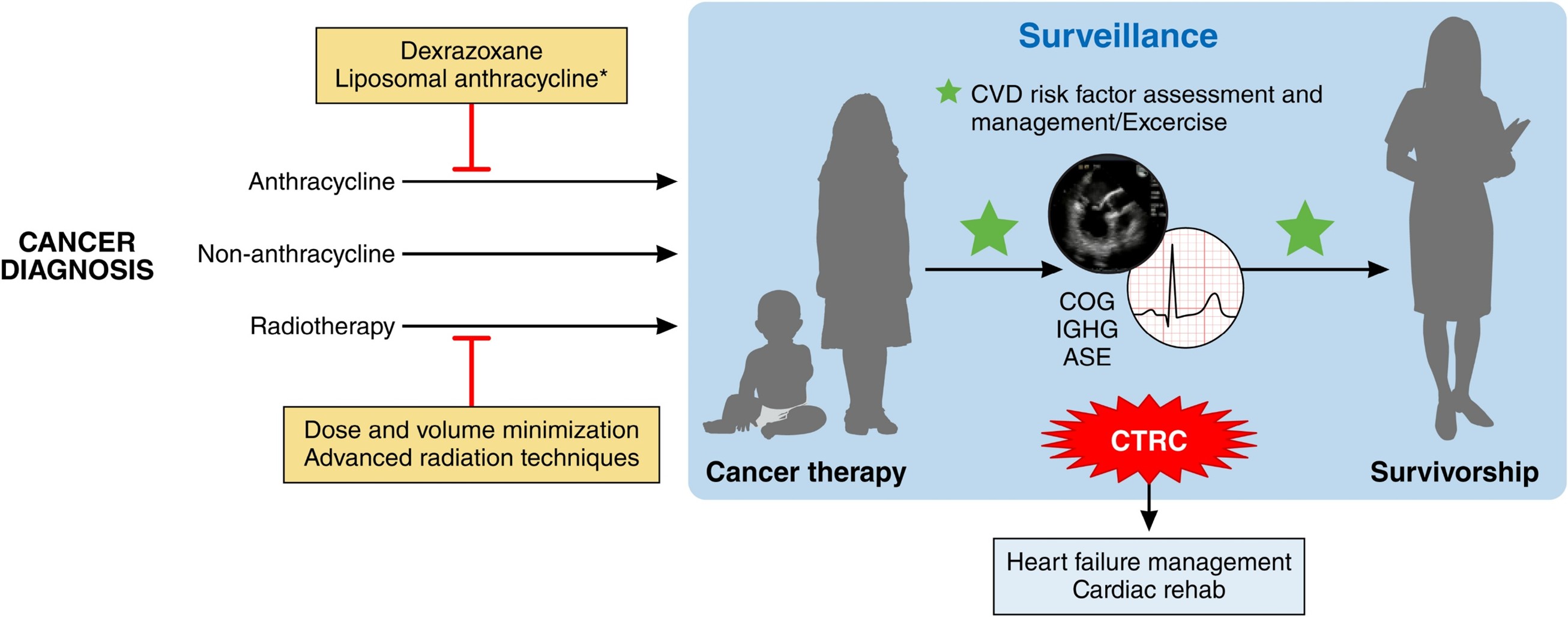
Reprinted with permission. Circulation.2025;151:e926-e943. ©2025 American Heart Association, Inc.
*Adult studies have demonstrated lower cardiomyopathy/HF risk with liposomal compared with standard anthracyclines, although definitive data in pediatrics are lacking.
ASE = American Society of Echocardiography; COG = Children's Oncology Group; CTRC = cancer treatment–related cardiotoxicity; CVD = cardiovascular disease; HF = heart failure; IGHG = International Guideline Harmonization Group; rehab = rehabilitation.
- Cardiometabolic considerations. Conventional CVD risk factors such as HTN, diabetes mellitus, and dyslipidemia are more prevalent and manifest earlier in long-term survivors of childhood cancer. Additionally, several cancer treatments are associated with the development of CVD risk factors (Figure 1). As such, the Children's Oncology Group (COG) Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancer recommend periodic screening of survivors for CVD risk factors.3
- Medical therapy and advanced cardiac therapies. Standard HF therapies have not been well studied in the management of children with cancer treatment–related CVD, and no formal guidelines exist beyond the 2023 AHA scientific statement on Treatment Strategies for Cardiomyopathy in Children, which includes discussion of cardio-oncology.4 Use of advanced cardiac therapies such as mechanical circulatory support and heart transplant are highly individualized to the patient and must consider the phase of treatment and risk of recurrence.
- Role of exercise. Multiple studies have demonstrated positive physical, psychological, and treatment effects of incorporating exercise throughout the course of cancer treatment. Exercise prescription in children should consider cardiopulmonary fitness and be adapted to accommodate any cancer treatment–related impairments. A formalized cardiac rehabilitation approach is recommended when available.
- Survivorship and transition of care. As patients age out of pediatric centers, a concerted effort must be placed on transition to appropriate adult providers for long-term care, including CV care if needed. As in the general population, health disparities are also evident in survivors of childhood cancer and should be a part of the equation of transition to adult care.
References
- Ryan TD, Bates JE, Kinahan KE, et al. Cardiovascular toxicity in patients treated for childhood cancer: a scientific statement from the American Heart Association. Circulation. 2025;151(15):e926-e943. doi:10.1161/CIR.0000000000001308
- Mertens L, Singh G, Armenian S, et al. Multimodality imaging for cardiac surveillance of cancer treatment in children: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2023;36(12):1227-1253. doi:10.1016/j.echo.2023.09.009
- Children's Oncology Group. Long-Term Follow-Up Guidelines for Survivors of Childhood, Adolescent, and Young Adult Cancer. Version 6.0 - October 2023 (Children's Oncology Group website). 2023. Available at: https://www.survivorshipguidelines.org/pdf/2025/COG_LTFU_Guidelines_Comprehensive_v6.pdf. Accessed 05/11/2026.
- Bogle C, Colan SD, Miyamoto SD, et al. Treatment strategies for cardiomyopathy in children: a scientific statement from the American Heart Association. Circulation. 2023;148(2):174-195. doi:10.1161/CIR.0000000000001151
Clinical Topics: Cardio-Oncology, Congenital Heart Disease and Pediatric Cardiology, Heart Failure and Cardiomyopathies
Keywords: Cardio-oncology, Survivorship, Cardiotoxicity, Pediatric Cardiology