Discontinuation of Oral Anticoagulation After AF Catheter Ablation (ALONE-AF): ALONE, but Not the Only One
Quick Takes
- ALONE-AF showed that discontinuation of oral anticoagulation (OAC) after catheter ablation of atrial fibrillation (AFCA) leads to a lower rate of a composite endpoint of stroke, systemic embolism, and major bleeding than continuing direct OAC in patients with an increased risk of stroke without documented recurrence of atrial arrhythmias in the first-year post-ablation.
- This trial adds to the evidence on OAC discontinuation after AFCA.
- Together with ODIn-AF and OCEAN, the ALONE-AF study opens the pathway for OAC discontinuation after AF ablation and supports relevant upcoming studies (POCKET-OAC, DIAMOND-AF, REACT-AF).
ALONE-AF Trial Description
The ALONE-AF (Anticoagulation One Year After Ablation of Atrial Fibrillation in Patients With Atrial Fibrillation) trial examined whether discontinuing oral anticoagulation (OAC) in patients with elevated stroke risk after catheter ablation of atrial fibrillation (AFCA) who remain free of atrial arrhythmias in the year after their indexed ablation leads to fewer adverse clinical outcomes.1
Methods
This was an open-label, randomized clinical trial conducted across 18 centers in South Korea. Patients with AF who underwent catheter ablation and remained free of recurrence of atrial arrhythmias after 1 year were randomized 1:1 to discontinue (n = 417) or continue OAC (n = 423) with apixaban or rivaroxaban. The primary endpoint was a composite of stroke, systemic embolism, or major bleeding.
Results
- In the intention-to-treat analysis at 2-year follow-up, the primary endpoint occurred in one patient (0.3%) in the discontinue OAC group and eight patients (2.2%) in the continue OAC group with an absolute difference of -1.9% (95% confidence interval [CI], -3.5 to -0.3; p= 0.02).
- Per-protocol analysis yielded similar estimates of 0.3% in the discontinue OAC group versus 2.3% in the continue OAC group with an absolute difference of -2.0% (95% CI, -3.7 to -0.3; p = 0.023).
- The number needed to treat via OAC discontinuation to prevent a primary outcome was 53 patients (95% CI, 29 to 333 patients).
- There was an insignificant difference in the cumulative incidence of stroke or systemic embolism at 2-year follow-up, occurring at a rate of 0.3% in the discontinue OAC group versus 0.8% in the continue OAC group (absolute difference, -0.5%; 95% CI, -1.6 to 0.6; p = 0.34) (Figure 1).
- There was a significant difference in major bleeding events, with no events occurring in the discontinue OAC group compared with five events (1.4%) in the continue OAC group, with an absolute difference of -1.4% (95% CI, -2.6 to -0.2; p = 0.03) at 2-year follow-up (Figure 1). One such event was a permanently disabling hemorrhagic stroke.
- Approximately 10% experienced AF recurrence and restarted anticoagulation.
- Clinically relevant nonmajor bleeding occurred in five patients (1.4%) in the no-OAC group versus seven patients (1.9%) in the OAC group.
- There were no reported cases of all-cause mortality or myocardial infarction.
Figure 1: ALONE-AF Trial Outcomes
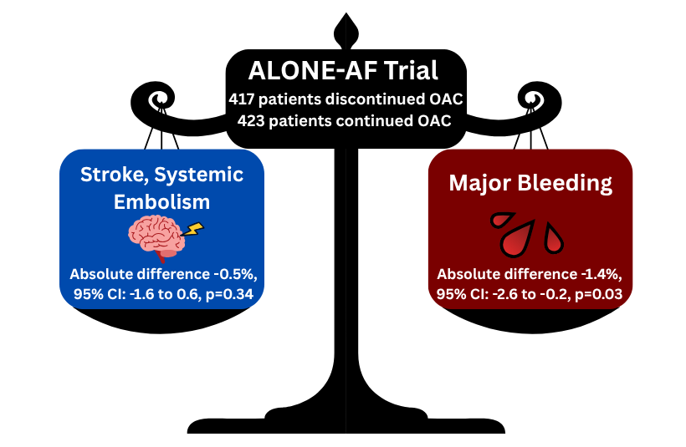
ALONE-AF = (Anticoagulation One Year After Ablation of Atrial Fibrillation in Patients With Atrial Fibrillation); CI = confidence interval; OAC = oral anticoagulation.
Conclusions
Discontinuation of OAC in patients with elevated stroke risk who remain free of atrial arrhythmias 1-year post-AFCA decreases the composite risk of stroke, systemic embolism, and major bleeding, largely due to a statistically significant decreased risk of bleeding with similar stroke rates compared with patients continued on OAC.
Perspective
ALONE-AF is a well-designed and well-executed study with clinically relevant findings. It provides continuing evidence to support the discontinuation of long-term anticoagulation in patients post-AFCA who remain free of atrial arrhythmias in the year following their indexed ablation. The absolute reduction in the primary endpoint (-1.9%, p = 0.02) seen without OAC is largely attributed to a lower rate of major bleeding events, with a similar rate of stroke noted regardless of OAC status. In subgroup analysis, however, a statistically significant difference was not seen among patients <65 years of age (46.9%) or in women (24.9%).
The trial has some limitations. The open-label design can introduce both ascertainment and reporting bias. The overall event rate was low and was skewed towards a higher absolute number of bleeding events or thromboembolic events, biasing the composite endpoint. Finally, in addition to a lower prevalence of women, most of the patient population was of East Asian descent, and only 30.5% of patients had a CHA2DS2-VASc score >2 (mean 2.1). Overall, these results reveal another clue in navigating the delicate balance of the risks and benefits conferred by anticoagulation in patients post-AFCA. More research is required prior to establishing clinical practice guidelines.
Together with the ODIn-AF (Prevention of Silent Cerebral Thromboembolism by Oral Anticoagulation With Dabigatran After Pulmonary Vein Isolation for Atrial Fibrillation) and OCEAN (Optimal Anticoagulation for Enhanced Risk Patients Post-Catheter Ablation for Atrial Fibrillation) trials, this study opens the pathway for OAC discontinuation after AF ablation and supports relevant upcoming studies.2,3 The ODIn-AF trial found no difference in cerebral embolic events when comparing OAC (dabigatran) to OAC discontinuation, in a population of patients with a mean CHA2DS2-VASc score of 2.6. The OCEAN trial found that in a population of patients with a mean CHA2DS2-VASc score of 2.2 and successful AFCA 1 year earlier, treatment with OAC (rivaroxaban) did not result in a significantly lower incidence of a composite of stroke, systemic embolism, or new covert embolic stroke than treatment with aspirin. Patients with a higher CHA2DS2-VASc score also have a higher thromboembolic and bleeding risk regardless of OAC intake,4 and have not been evaluated extensively in randomized trials yet.
The ALONE-AF trial supports emerging evidence for OAC discontinuation after successful AFCA. Ongoing and upcoming trials are evaluating individualized OAC management guided by documented AF recurrences, detected through continuous rhythm monitoring using implantable loop recorders (e.g., POCKET-OAC [Pill-in-the-POCKET Oral Anticoagulation Strategy After AF Catheter Ablation]) or wearable technologies such as smartwatches (e.g., DIAMOND-AF [Discontinuation of Anticoagulation With Intensive Rhythm Monitoring in Post-Ablation Patients With Atrial Fibrillation] and REACT-AF [Rhythm Evaluation for AntiCoagulaTion with Continuous Monitoring of Atrial Fibrillation]). These results have the potential to inform future guideline updates and significantly influence contemporary clinical practice.
References
- Kim D, Shim J, Choi EK, et al. Long-term anticoagulation discontinuation after catheter ablation for atrial fibrillation: the ALONE-AF randomized clinical trial. JAMA. 2025;334(14):1246-1254. doi:10.1001/jama.2025.14679
- Schrickel JW, Beiert T, Linhart M, et al. Prevention of cerebral thromboembolism by oral anticoagulation with dabigatran after pulmonary vein isolation for atrial fibrillation: the ODIn-AF trial. Clin Res Cardiol. 2024;113(8):1183-1199. doi:10.1007/s00392-023-02319-9
- Verma A, Birnie DH, Jiang C, et al. Antithrombotic therapy after successful catheter ablation for atrial fibrillation. N Engl J Med. 2026;394(4):323-332. doi:10.1056/NEJMoa2509688
- Oda Y, Nogami A, Komatsu Y, et al. Assessment of long-term use versus discontinuation of direct oral anticoagulant after catheter ablation for atrial fibrillation-RYOUMA Registry subanalysis. Ann Noninvasive Electrocardiol. 2025;30(3):e70067. doi:10.1111/anec.70067
Clinical Topics: Anticoagulation Management, Arrhythmias and Clinical EP, Anticoagulation Management and Atrial Fibrillation, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias
Keywords: Atrial Fibrillation, Catheter Ablation, Anticoagulation Management, Anticoagulants, ESC25, ESC Congress