ALLEVIATE-HF: ICM-Based HF Risk Detection and CV Outcomes; Arrythmia Burden
Heart failure (HF) risk detection with an insertable cardiac monitor (ICM) paired with a centrally coordinated nurse-led diuretic intervention was safe but did not reduce cardiovascular events in ambulatory patients with recent symptomatic HF events, according to findings from the ALLEVIATE-HF trial published May 27 in JACC.
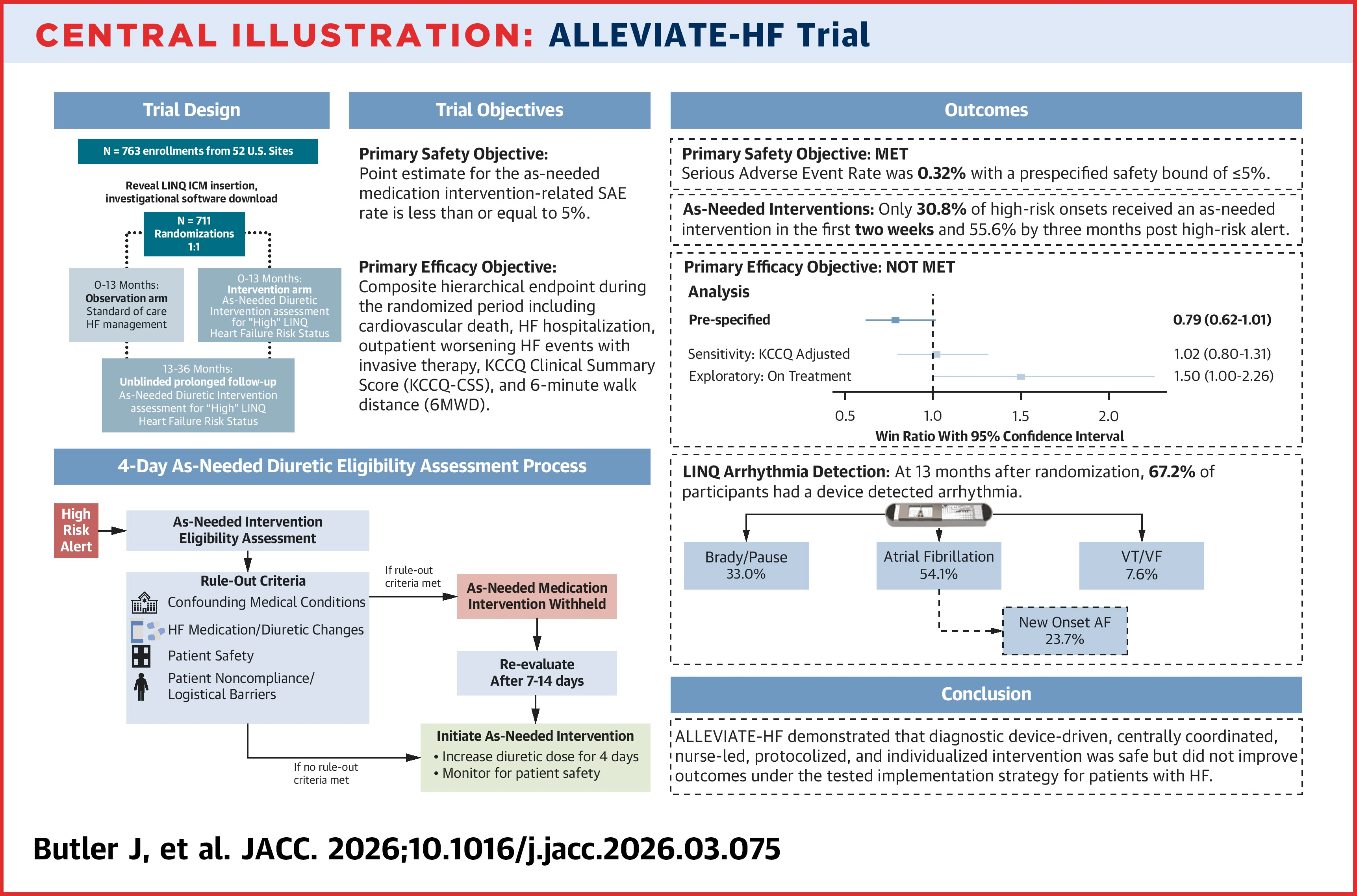
In the prospective, double-blind trial, conducted between September 2020 and June 2025 at 52 U.S. sites, Javed Butler, MD, MPH, MBA, FACC, et al., implanted a Reveal LINQ subcutaneous ICM in 711 patients (71 years; 46% women) and randomized them to either observation with standard care (n=354) or intervention (n=357).
Eligible patients had NYHA class II-III symptoms, HF hospitalization within 12 months, intravenous HF therapy within six months or elevated natriuretic peptides within three months of enrollment.
Of the enrolled patients, 68% had heart failure with preserved ejection fraction (HFpEF) and 32% had heart failure with reduced ejection fraction (HFrEF); 76% had atrial fibrillation (AFib)/flutter/tachycardia. Baseline characteristics were mostly well balanced between groups, although in the intervention group vs. the control group the rate of prior myocardial infarction was higher (24% vs. 16; p=0.011) as well as the Kansas City Cardiomyopathy Questionnaire Clinical Summary Score (KCCQ-CSS) (66.2 vs. 63.1; p=0.018).
The intervention consisted of a prespecified, self-administered four-day diuretic intensification pathway triggered by a HF high-risk status alert and facilitated by a centralized nursing team if there were no rule-out conditions.
Results over a mean follow-up of 17.3 months showed that 426 of all participants experienced at least one high-risk alert: 62% in the observation arm and 58% in the intervention arm.
Of 931 interventions, only three were associated with an as-needed medication-related serious adverse event (0.32%), falling within the prespecified safety threshold of ≤5%.
However, there were no significant differences between the two arms in terms of the primary efficacy endpoint – a 5-component hierarchal composite of cardiovascular death or HF hospitalization or outpatient HF event within 60 days of high-risk onset, KCCQ-CSS, and six-minute walk distance (win ratio, 0.79; p=0.06), with an exploratory sensitivity analysis adjusting for baseline KCCQ-CSS imbalance yielding a similar win ratio of 1.02 (p=0.85). Cumulative cardiovascular death and HF events were numerically higher in the intervention arm (hazard ratio [HR], 1.43).
"Although the approach in this trial was safe, the lack of benefit may be related to an overly conservative approach," write Butler, et al. Only 31% of first high-risk alerts were followed by treatment within 14 days, and only 64% of high-risk alert-triggering patients received the therapy within six months. Of the 80 cardiovascular death or HF events in the intervention arm that were preceded by a high-risk event, most (83%) were not treated within 14 days – the most common reasons being recent HF medication change and confounding medical conditions.
"A key lesson from the ALLEVIATE-HF trial is that alerts are not treatment, and signals without a timely response lose their clinical impact," write Tariq Ahmad, MD, FACC, and Andrew J. Sauer, MD, in an accompanying editorial comment. "Future studies should stop treating the alert as the intervention and instead define the alert-to-action pathway as the true intervention. That means prespecifying process metrics such as acknowledgment time, response time, proportion of alerts acted on within 48 to 72 hours, override frequency, reasons for deferral, and completion of escalation steps."
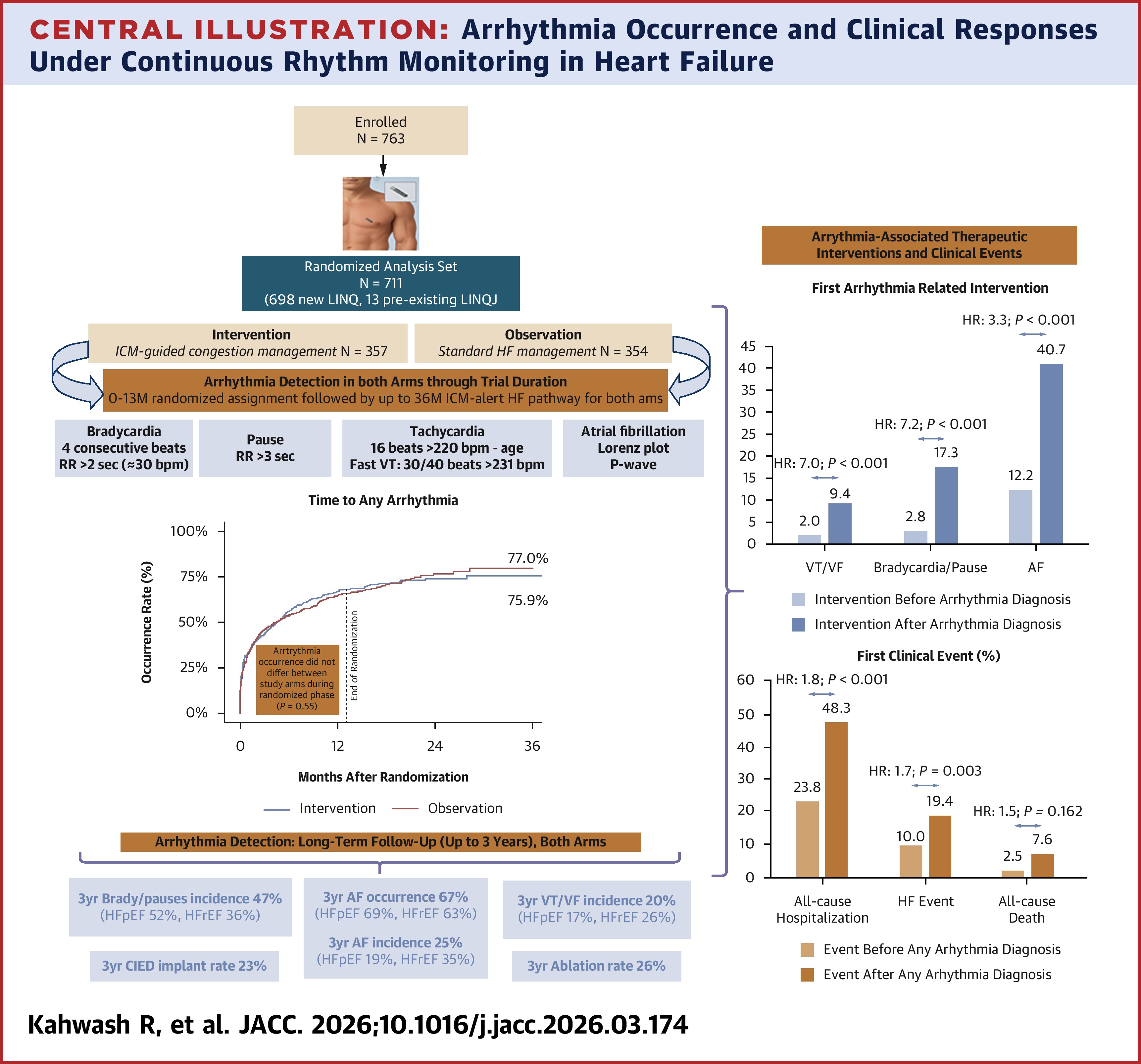
In the same issue of JACC, a secondary observational analysis of the ALLEVIATE-HF cohort found that the ICM intervention had no effect on arrythmia burden but yielded new insight into the association between clinically meaningful arrhythmias, clinical events and therapeutic interventions.
Results showed that during the 13-month randomized phase, the rates of arrythmia did not differ between the two arms, with substantial arrythmia burden in both during the prolonged follow-up. The overall occurrence of AFib at three years was 67% and the incidence of new-onset AFib was 25%.
Bradyarrhythmia occurred in 47% of participants, and ventricular tachycardia or fibrillation (VT/VF) in 20%. The rate of implanting cardiac implantable electronic devices was 23%, and ablation was 26%.
Presence of any arrythmia was associated with a subsequent increase in arrythmia-related interventions (HR, 3.81), for VT/VF (HR, 7.04) and bradyarrhythmia (HR, 7.22), as well as AFib (HR, 3.28; p<0.001 for all). It was also associated with an increased risk of all-cause hospitalization (HR, 1.79; p<0.001) and HF events (HR, 1.69; p=0.003).
Bradyarrhythmias and pauses were more frequent in patients with HFpEF than HFrEF (52% vs. 36%), while VT/VF events tended to occur more often in patients with HFrEF.
"These findings may highlight the diagnostic value of continuous rhythm surveillance in HF, while emphasizing the need for further investigations to determine whether arrhythmia detection-guided interventions improve clinical outcomes in chronic HF," conclude study authors Rami Kahwash, MD, et al.
"ALLEVIATE-HF provides provocative data on the epidemiology, natural history, and burden of arrhythmias in a diverse HF population," write Mark N. Belkin, MD, FACC; Natalie Van Ochten, MD; and Gaurav A. Upadhyay, MD, FACC, in an accompanying editorial comment. "Trials are now needed to address how monitoring improves arrhythmia detection over routine clinical care and, more important, which interventions should be used to prevent rather than treat arrhythmia and lead to improved patient outcomes."
Citations:
- Butler, J, Kahwash, R, Khan, M. et al. Risk-Based Nurse-Managed Personalized Heart Failure Interventions: The ALLEVIATE-HF Trial. JACC. Published online, May 27, 2026. doi: 10.1016/j.jacc.2026.03.075
- Kahwash, R, Butler, J, Khan, M. et al. Arrhythmia Burden and Clinical Responses Under Continuous Monitoring in Heart Failure: Observations From the ALLEVIATE-HF Trial. JACC. Published online, May 27, 2026. doi: 10.1016/j.jacc.2026.03.174
Clinical Topics: Arrhythmias and Clinical EP, Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Acute Heart Failure
Keywords: Tachycardia, Ventricular, Atrial Fibrillation, Diuretics, Heart Failure, Bradycardia