FLOW Analysis: Semaglutide Delivers Consistent Kidney Benefit in T2D/CKD Across CVD Status
Semaglutide improved kidney and survival outcomes in patients with type 2 diabetes (T2D) and chronic kidney disease (CKD), including those with established atherosclerotic cardiovascular disease (ASCVD), heart failure (HF) and high total cardiovascular disease risk, according to a subgroup analysis of the FLOW trial published June 2 in JACC.
A total of 3,533 patients were randomized to once-weekly subcutaneous semaglutide 1.0 mg or placebo. They were 67 years old and a third were women; their mean estimated glomerular filtration rate (eGFR) was 47.0 mL/min/1.73 m2 and median urine albumin-to-creatinine ratio (UACR) was 568 mg/g.
Of the participants, 34% had ASCVD (prior myocardial infarction [MI], stroke or peripheral artery disease), 20% had HF and 67% were at high cardiovascular risk (PREVENT score ≥20%) without existing cardiovascular disease.
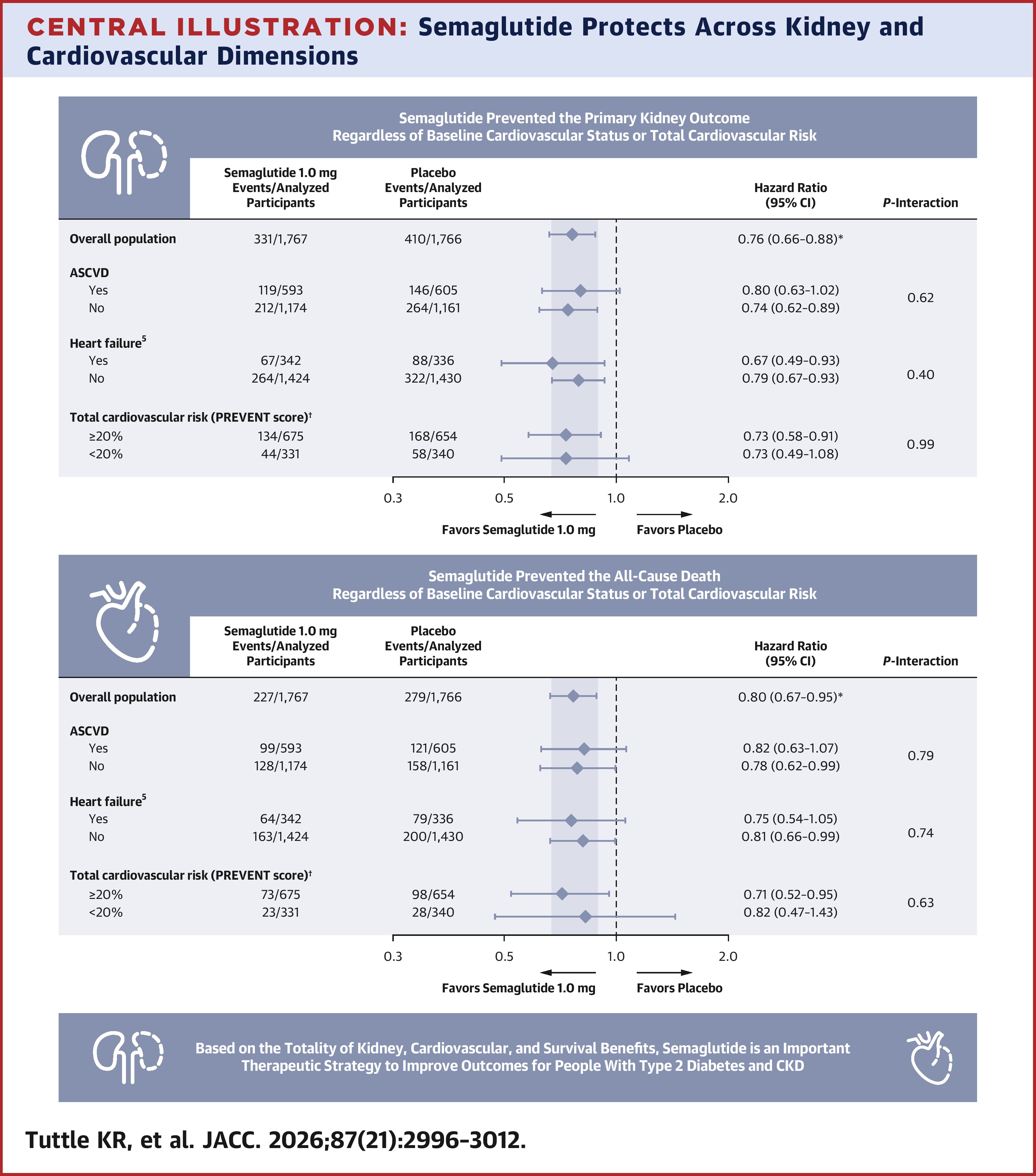
Results in the overall cohort showed that semaglutide reduced the risk of the primary outcome (≥50% eGFR decline, eGFR <15 mL/min/1.73 m2, dialysis, transplantation and kidney or cardiovascular death) by 24% and all-cause death by 20%.
This benefit was consistent within the groups with and without ASCVD (hazard ratio [HR], 0.80 vs. HR, 0.74; pint=0.62), with and without HF (HR, 0.67 vs. HR, 0.79; pint = 0.40) and with and without high total cardiovascular disease risk (HR, 0.73 for both; pint= 0.99).
Numbers needed to treat to prevent one primary kidney outcome at three years were 22, 13 and 17, within the ASCVD, HF and high-risk groups, respectively.
Similarly, semaglutide reduced the risk of all-cause death in patients with and without ASCVD (HR, 0.82 vs. HR, 0.78), with and without HF (HR, 0.75 vs. HR, 0.81) and with and without high total cardiovascular disease risk (HR, 0.71 vs. HR, 0.82).
"Considering the high absolute rates of major adverse kidney events and death across subgroups with cardiovascular disease or at high total cardiovascular disease risk, the clinical impact of semaglutide treatment is especially important for these individuals," write analysis authors Katherine R. Tuttle, MD, et al.
"Taken together, the results from this analysis represent a key opportunity to intensify [cardiovascular] kidney therapies in real-world practice in high-risk CKD even without overt [cardiovascular disease] being present, given comparable event rates and benefits from therapies," add Janani Rangaswami, MD; James L. Januzzi, MD, FACC; and Roy O. Mathew, MD, in an accompanying editorial comment. "Implementing therapies that demonstrate [cardiovascular]-kidney benefits, and especially those that can change the trajectory of kidney function decline must be prioritized as a primary [cardiovascular disease] optimization strategy."
Clinical Topics: Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Diabetes Mellitus, Type 2, Renal Insufficiency, Chronic, Semaglutide, Heart Failure