SHaRe Registry Identifies MACE Predictors in Mild HCM
About one in five patients with phenotypically mild hypertrophic cardiomyopathy (HCM) experienced major adverse cardiovascular events (MACE) over seven years of follow-up, according to SHaRe Registry research published July 8 in JACC. Older age, symptom progression and increases in left atrial (LA) diameter, left ventricular (LV) hypertrophy and LV outflow tract (LVOT) gradient were among the strongest predictors of risk.
To understand the natural history of phenotypically mild HCM, as well as risk predictors and potential management strategies, Constantin-Cristian Topriceanu, MBBS, PhD, et al., followed 2,500 participants in the SHaRe Registry (about 20% of total participants in the international registry) to assess the occurrence of MACE – atrial fibrillation (AFib), malignant ventricular arrhythmia (MVA), heart failure (HF), stroke or all-cause mortality. Their mean age was 43 years, and 31% were women.
Phenotypically mild HCM was defined as short disease duration (<10 years since diagnosis or age ≤30 years), no prior MACE, NYHA class I symptoms and LV maximal wall thickness (MWT) <25 mm.
During a median follow-up of seven years, 534 participants (21%) developed MACE, including 289 with AFib, 69 with MVA (sudden cardiac death, resuscitated arrest or appropriate defibrillator therapy) and 193 with HF (cardiac transplantation, LV assist device implantation, LVEF <35% or NYHA functional class III or IV). Symptom progression was also common: 585 participants (23%) progressed from NYHA class I to class II or higher and were 2.79-times more likely to experience MACE.
Baseline predictors of MACE included age (hazard ratio [HR], 1.24 per 10-year increase); female sex; BMI (HR, 1.10 per 5-kg/m2 increase); LA diameter (HR, 1.16 per 5-mm increase); LV MWT (HR, 1.27 per 5-mm increase) and LVOT gradient (HR, 1.08 per 15-mm Hg increase). Presence of LV late gadolinium enhancement was associated with a 36% higher risk of MACE.
Higher sustained values or steeper increases in LA diameter, LV MWT and LVOT gradient were associated with the highest rate of MACE. Increases in LA diameter were associated with higher AFib and HF rates, while steeper increases in LV MWT were associated with higher MVA rates.
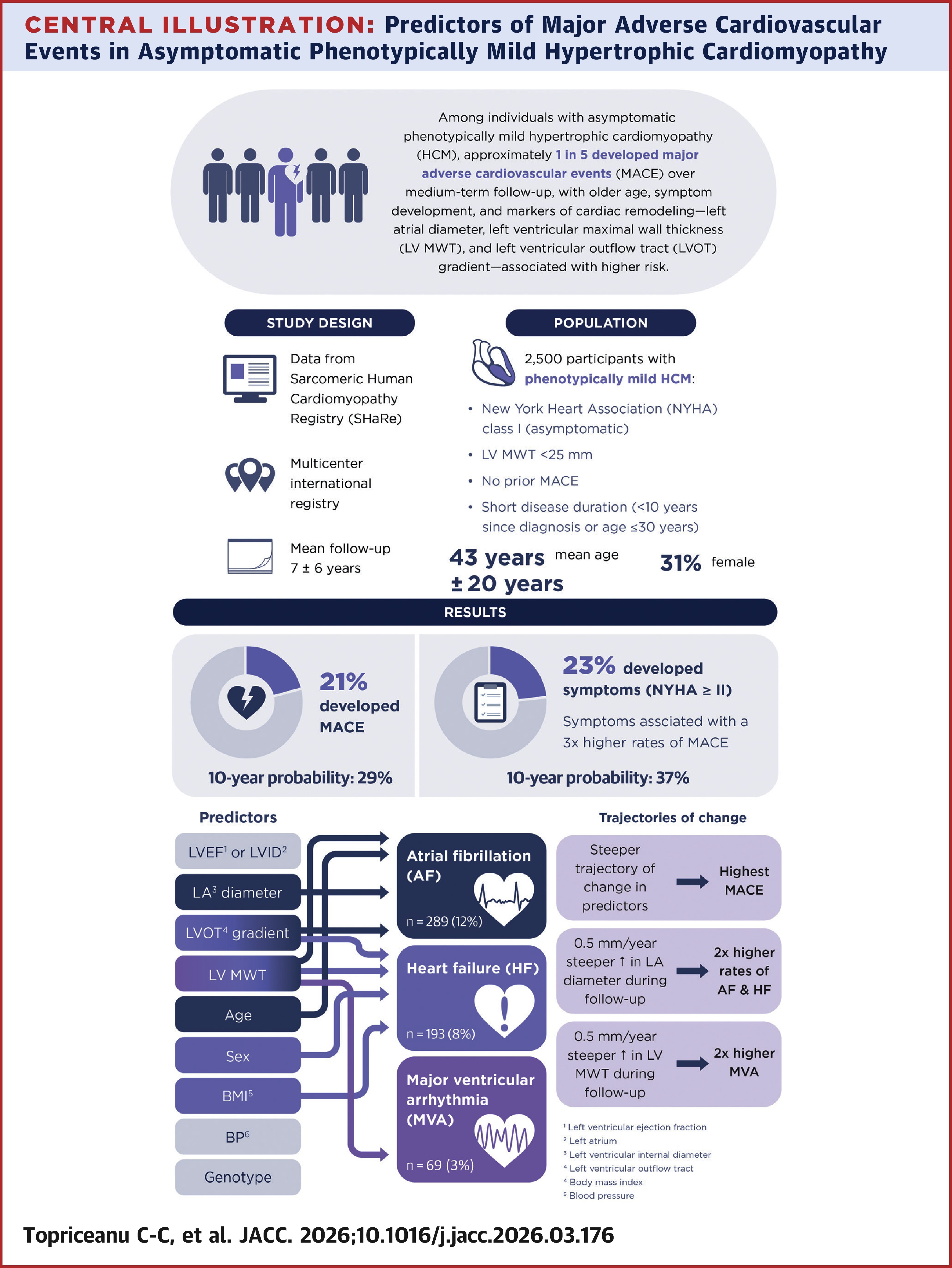
"These findings may help identify higher-risk patients earlier in their clinical journey, guide outpatient management strategies, and inform participant selection, sample size calculations, and endpoint definition for future clinical trials evaluating novel disease-modifying therapies," the authors write.
"These data demonstrate the power of long-term, coordinated, multicenter registries such as SHaRe to identify the driving factors in complex, slowly progressing pathology and identify characteristic features of a range of clinical trajectories," write Mark W. Russell, MD, and Joshua K. Meisner, MD, PhD, in an accompanying editorial comment. "Partnering risk modeling with potential disease-modifying therapies holds tremendous promise for improving care for patients with HCM."
Clinical Topics: Arrhythmias and Clinical EP, Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Atrial Fibrillation/Supraventricular Arrhythmias, Acute Heart Failure
Keywords: Cardiomyopathy, Hypertrophic, Cardiomyopathies, Atrial Fibrillation, Heart Failure