A 60-year-old patient who is a prior heavy smoker and actively receiving paclitaxel 40 mg intravenously weekly, carboplatin 210 mg intravenously weekly, and volumetric modulated arc radiotherapy (40 out of 60 Gy) to the right upper chest presented with fever of 100.5 following radiation therapy. She has a past medical history of stage 4 (T1 N2 M1) spindle cell lung cancer with prior gamma knife radiosurgery, asthma/chronic obstructive pulmonary disease, diabetes mellitus type 2, and major depression. She was hypotensive with systolic blood pressure in the 80s at the time. She was asymptomatic, not noting any palpitations, lightheadedness, or dizziness, though she was notably depressed and generally sedentary. No source of infection was identified. Active medications include oxycodone, prochlorperazine, duloxetine, levetiracetam, and clonazepam. Figure 1 shows the rhythm found upon placing on telemetry. Figure 2 shows stable electrocardiogram.
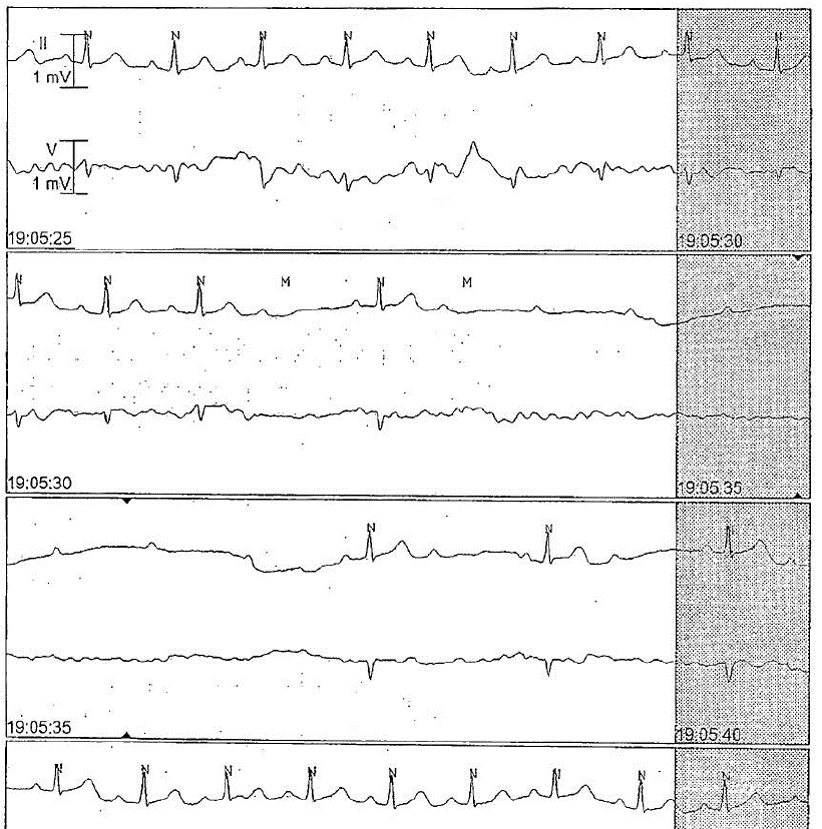
Figure 1
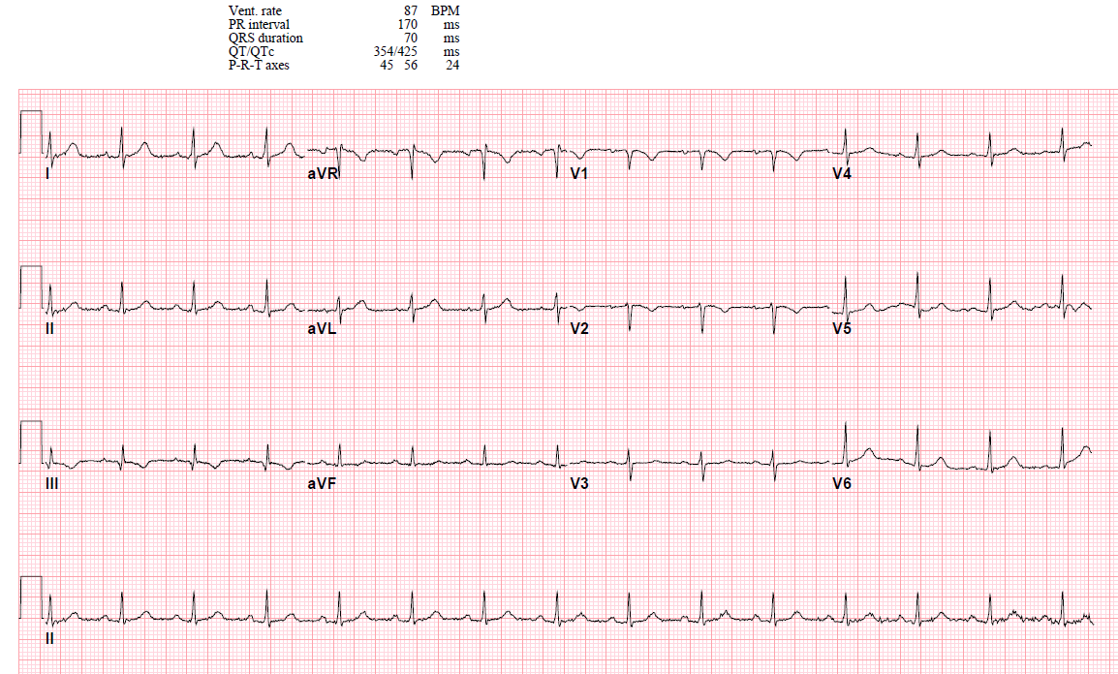
Figure 2
The correct answer is: D. Paclitaxel; monitor and consider finding alternative agent
This patient likely has paclitaxel-induced heart block. She has no history of coronary artery disease and no electrocardiographic changes consistent with prior ischemia/infarction. The heart block was discovered incidentally and was asymptomatic, though with a notable decrease in blood pressure. Vagal stimulation is less likely in the setting of being completely asymptomatic with no obvious trigger. Gamma knife surgery or other radiotherapy may alter the autonomic system, but it would be more in the direction of vagal suppression and not cause heart block.1 Although uncommon, paclitaxel has been known to cause heart block since the 1990s, and this can occur up to days after the infusion.2 Generally speaking, these patients are asymptomatic and respond to ceasing the agent after 24-72 hours, as did our patient. In a meta-analysis of 140 patients receiving paclitaxel from 3 phase I trials and 1 phase II trial, bradycardia was surprisingly common, with an incidence of 29%. The incidence of more significant arrhythmias was 4.3%, of which 1.4% were heart block. The mechanism of the bradyarrhythmias is largely unknown but is suspected to be related to the indirectly reduced sodium channel function by tubulin polymerization.3 Placing a pacemaker in this patient would not be indicated and would potentially carry unnecessary risk because she has active cancer and has ongoing chest radiotherapy.
References
- Hoca A, Yildiz M, Ozyigit G. Evaluation of the effects of mediastinal radiation therapy on autonomic nervous system. Med Oncol 2012;29:3581-6.
- Rowinsky EK, McGuire WP, Guarnieri T, Fisherman JS, Christian MC, Donehower RC. Cardiac disturbances during the administration of taxol. J Clin Oncol 1991;9:1704-12.
- Casini S, Tan HL, Demirayak I, et al. Tubulin polymerization modifies cardiac sodium channel expression and gating. Cardiovasc Res 2010;85:691-700.