A 49-year-old female high school teacher is referred for evaluation of hypertrophic cardiomyopathy (HCM). She had presented to her primary care provider with symptoms of mild exertional angina and dyspnea. A transthoracic echocardiogram is obtained and reveals increased left ventricular (LV) wall thickness concerning for HCM.
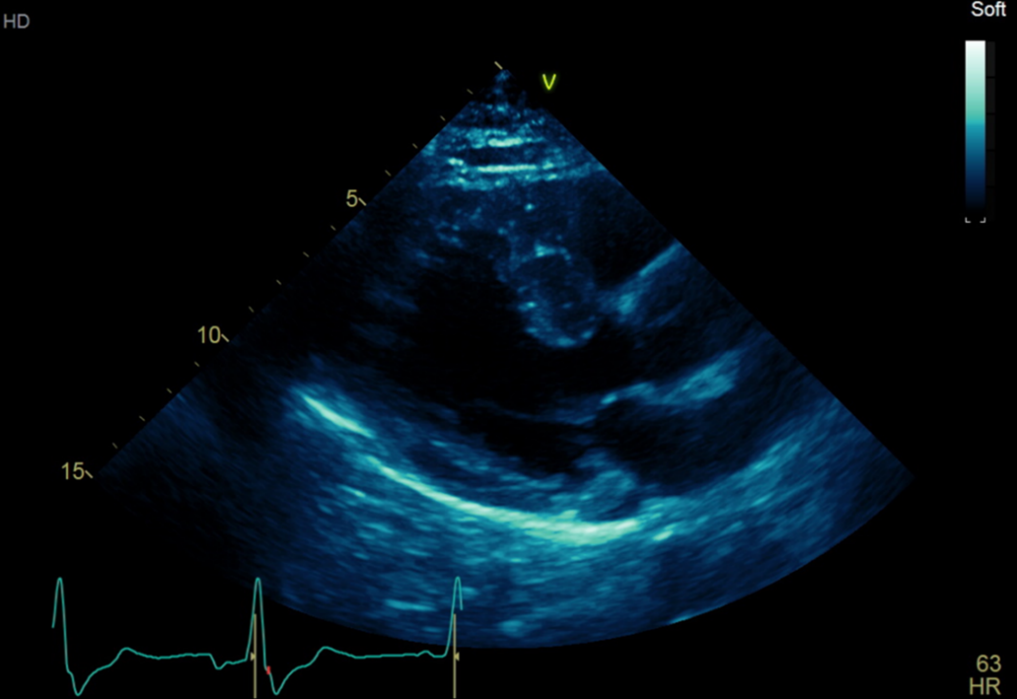
Vital signs included heart rate 72 bpm and blood pressure 121/82 mm Hg. Her body mass index is 24 kg/m2. Physical examination reveals a grade 2/6 crescendo–decrescendo systolic murmur at the lower left sternal border that increases to a grade 4/6 with Valsalva. Lungs are clear to auscultation and there is no lower extremity edema. A repeat transthoracic echocardiogram reveals ejection fraction 61%, increased LV wall thickness with asymmetric involvement of the septum extending to the apex, systolic anterior motion (SAM) of the mitral valve with obstruction, and secondary mitral regurgitation (MR), which is severe. The maximal LV wall thickness is measured at 15 mm (Figure 1), and a maximal instantaneous Doppler gradient in the left ventricular outflow tract (LVOT) is measured at 90 mm Hg.
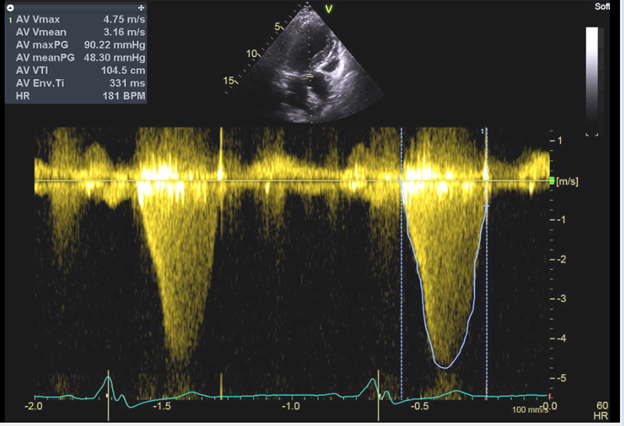
Figure 1: Transthoracic echocardiogram showing the left ventricle in the parasternal long axis view. A, The thickened ventricular septum measuring 15 mm. B, Continuous wave Doppler assessment through the aortic valve with a peak gradient measuring 90 mmHg.
Figure 1A
Figure 1: Transthoracic echocardiogram showing the left ventricle in the parasternal long axis view. A, The thickened ventricular septum measuring 15 mm. B, Continuous wave Doppler assessment through the aortic valve with a peak gradient measuring 90 mmHg.
Figure 1B
Figure 1: Transthoracic echocardiogram showing the left ventricle in the parasternal long axis view. A, The thickened ventricular septum measuring 15 mm. B, Continuous wave Doppler assessment through the aortic valve with a peak gradient measuring 90 mmHg.
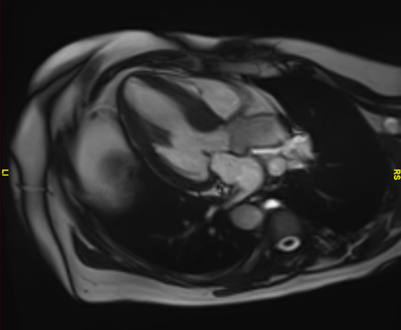
She is initiated on beta-blocker therapy with metoprolol succinate 25 mg daily. A 24-hour ambulator monitor does not reveal any arrhythmias, including absence of ventricular tachycardia. A cardiac magnetic resonance imaging confirms LV asymmetric hypertrophy with a sigmoid-shaped septum measuring up to 18 mm (Figure 2).
Figure 2: Cardiac magnetic resonance imaging confirming the presence of an asymmetric thickened ventricular septum measuring 18 mm.
Figure 2
Figure 2: Cardiac magnetic resonance imaging confirming the presence of an asymmetric thickened ventricular septum measuring 18 mm.
At her 1-month follow-up visit, she reports worsening angina, particularly after meals, and worsening shortness of breath with minimal exertion despite compliant use of a beta-blocker. Heart rates at home have been consistently around 60 bpm. Her physical examination and repeat echocardiogram confirm that the systolic murmur and LVOT gradient are both unchanged.
Which one of the following is the best next step for the management of this patient's symptoms?
Show Answer
The correct answer is: C. Refer the patient to a comprehensive center for consideration of septal myectomy.
The most appropriate answer choice for this patient is answer choice C. Due to her continued symptoms of dyspnea and angina despite medical therapy with beta-blockers, it is a Class I recommendation to refer this patient to an experienced center for consideration for surgical myectomy. Per the 2020 American Heart Association/American College of Cardiology (AHA/ACC) Guideline for the Diagnosis and Treatment of Patients With HCM, surgical myectomy is an appropriate treatment option for obstructive HCM that is refractory to medical therapy.1-4 Surgical myectomy can also reduce or eliminate SAM-mediated MR, which can lead to adverse remodeling of the LV and left atrium over time.5-8 This procedure has a mortality of <1% and success rate of approximately 90-95% when performed at experienced centers.8-12
Alcohol septal ablation (ASA) carries a Class I indication for patients with persistent symptoms despite medical therapy in whom surgery is contraindicated due to high surgical risk. As this patient had no contraindications for surgical procedures, surgical myectomy would be more appropriate than ASA, making answer choice D an incorrect choice. Although techniques for ASA have improved, this procedure may be less effective in patients with high resting gradients (≥100 mm Hg) and extreme septal thickness (≥30 mm).13,14 ASA is associated with a greater risk of conduction block requiring permanent pacemaker compared with surgical myectomy. In addition, there is a greater likelihood for repeat interventions due to residual gradients following ASA in 7-20% of patients.13,15,16
Answer choice A is an incorrect choice because the patient's heart rate was reported to be approximately 60 bpm while on beta-blocker therapy. Therefore, further uptitration of beta-blocker therapy would not be appropriate.
For answer choice B, it is a Class I recommendation to trial nondihydropyridine calcium channel blockers in patients with obstructive HCM and symptoms attributable to left ventricular outflow tract obstruction (LVOTO) in whom beta-blocker therapy has been ineffective or not tolerated. These medications have vasodilating properties that make them a reasonable option for treatment of LVOTO in patients with concomitant hypertension. However, the afterload-reducing effects of these medications can be dangerous in patients with high resting gradients and signs of heart failure. Although this patient did not exhibit signs or symptoms of heart failure, she had a high resting gradient and normotension. Therefore, the afterload-reducing effects of nondihydropyridine calcium channel blockers could further exacerbate her degree of obstruction, making answer choice B an incorrect choice.
This patient subsequently undergoes surgical myectomy without residual LVOTO. She then returns to her job as a teacher and can perform moderate-intensity exercise without symptoms of shortness of breath or angina.
Educational grant support provided by: Bristol Myers Squib To visit the course page for the Hypertrophic Cardiomyopathy: Accelerating Guideline-Driven Care grant, click here.
References
Hang D, Schaff HV, Ommen SR, Dearani JA, Nishimura RA. Combined transaortic and transapical approach to septal myectomy in patients with complex hypertrophic cardiomyopathy. J Thorac Cardiovasc Surg 2018;155:2096-102.
Kunkala MR, Schaff HV, Nishimura RA, et al. Transapical approach to myectomy for midventricular obstruction in hypertrophic cardiomyopathy. Ann Thorac Surg 2013;96:564-70.
Nguyen A, Schaff HV. Surgical myectomy: subaortic, midventricular, and apical. Cardiol Clin 2019;37:95-104.
Ommen S, Mital S, Burke M, et al. 2020 ACC/AHA guideline for the diagnosis and treatment of patients with hypertrophic cardiomyopathy: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2020;76:3022-55.
Deb SJ, Schaff HV, Dearani JA, Nishimura RA, Ommen SR. Septal myectomy results in regression of left ventricular hypertrophy in patients with hypertrophic obstructive cardiomyopathy. Ann Thorac Surg 2004;78:2118-22.
Hang D, Schaff HV, Nishimura RA, et al. Accuracy of jet direction on Doppler echocardiography in identifying the etiology of mitral regurgitation in obstructive hypertrophic cardiomyopathy. J Am Soc Echocardiograph 2019;32:333-40.
Hong JH, Schaff HV, Nishimura RA, et al. Mitral regurgitation in patients with hypertrophic obstructive cardiomyopathy: implications for concomitant valve procedures. J Am Coll Cardiol 2016;68:1497-504.
Nguyen A, Schaff HV, Nishimura RA, et al. Does septal thickness influence outcome of myectomy for hypertrophic obstructive cardiomyopathy? Eur J Cardiothorac Surg 2018;53:582-9.
Balaram SK, Ross RE, Sherrid MV, et al. Role of mitral valve plication in the surgical management of hypertrophic cardiomyopathy. Ann Thorac Surg 2012;94:1990-7; discussion 1997-8.
Hodges K, Rivas CG, Aguilera J, et al. Surgical management of left ventricular outflow tract obstruction in a specialized hypertrophic obstructive cardiomyopathy center. J Thorac Cardiovasc Surg 2019;157:2289-99.
Maron BJ, Dearani JA, Ommen SR, et al. Low operative mortality achieved with surgical septal myectomy: role of dedicated hypertrophic cardiomyopathy centers in the management of dynamic subaortic obstruction. J Am Coll Cardiol 2015;66:1307-8.
Rastegar H, Boll G, Rowin EJ, et al. Results of surgical septal myectomy for obstructive hypertrophic cardiomyopathy: the Tufts experience. Ann Cardiothorac Surg 2017;6:353-63.
Nguyen A, Schaff HV, Hang D, et al. Surgical myectomy versus alcohol septal ablation for obstructive hypertrophic cardiomyopathy: a propensity score-matched cohort. J Thorac Cardiovasc Surg 2019;157:306-315.e3.
Sorajja P, Binder J, Nishimura RA, et al. Predictors of an optimal clinical outcome with alcohol septal ablation for obstructive hypertrophic cardiomyopathy. Catheter Cardiovasc Interv 2013;81:E58-67.
Batzner A, Pfeiffer B, Neugebauer A, Aicha D, Blank C, Seggewiss H. Survival after alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy. J Am Coll Cardiol 2018;72:3087-94.
Kimmelstiel C, Zisa DC, Kuttab JS, et al. Guideline-based referral for septal reduction therapy in obstructive hypertrophic cardiomyopathy is associated with excellent clinical outcomes. Circ Cardiovasc Interv 2019;12:doi: 10.1161/CIRCINTERVENTIONS.118.007673.