Cardiac MRI in the Diagnosis of Arrhythmogenic Cardiomyopathy
A 60-year-old woman with a medical history of migraine headaches is referred for evaluation of recurrent syncope and presyncope. She has a history of syncope since high school. Her most recent episode of syncope was in August 2023, 18 months before her evaluation. This episode occurred while sitting and speaking with her daughters in the setting of a severe headache. She had no other prodromal symptoms and lost consciousness for <1 min. She has had episodes of presyncope while driving that prompted her to pull over to the side of the road. She has not had exertional syncopal episodes.
On evaluation, an electrocardiogram (ECG) demonstrates premature ventricular complexes (PVCs; left bundle branch block pattern; originating in the right ventricle [RV]) and T-wave inversion (TWI) in leads V1 through V3 without evidence of epsilon waves (Images 1, 2). A loop recorder that is implanted later demonstrates frequent premature atrial complexes, frequent PVCs, and short runs of nonsustained ventricular tachycardia (otherwise sinus bradycardia). An echocardiogram at an outside hospital demonstrates RV dilation, moderately reduced systolic function, and mild to moderate tricuspid regurgitation, per report. There is normal left ventricular (LV) systolic and diastolic function and no significant left-sided valvular heart disease, per report. Subsequent right heart catheterization demonstrates normal pulmonary artery pressures and pulmonary vascular resistance.
Image 1: ECG Tracing Demonstrating TWIs in Leads V1 Through V3 and PVCs
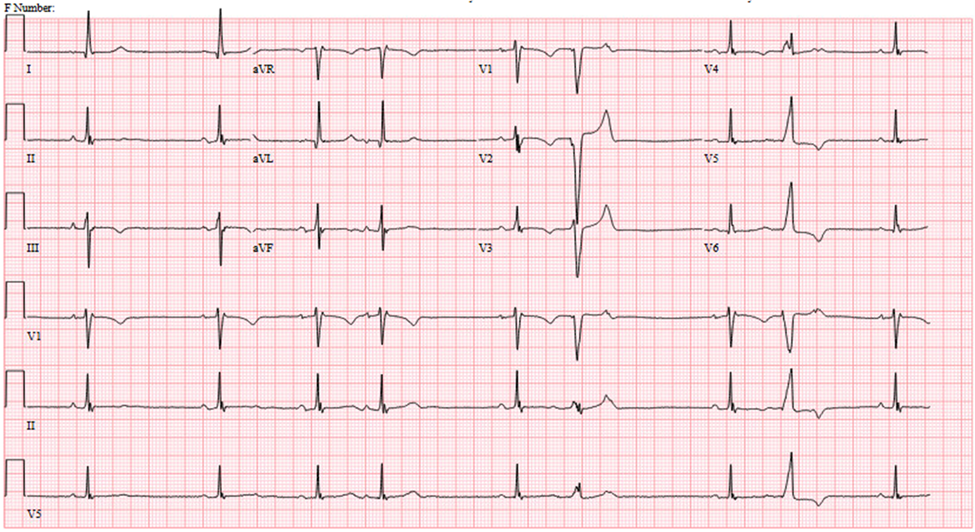
ECG = electrocardiogram; PVC = premature ventricular complex; TWI = T-wave inversion.
Image 2: Rhythm Strip Demonstrating PVCs Originating From the RVOT and RV Free Wall
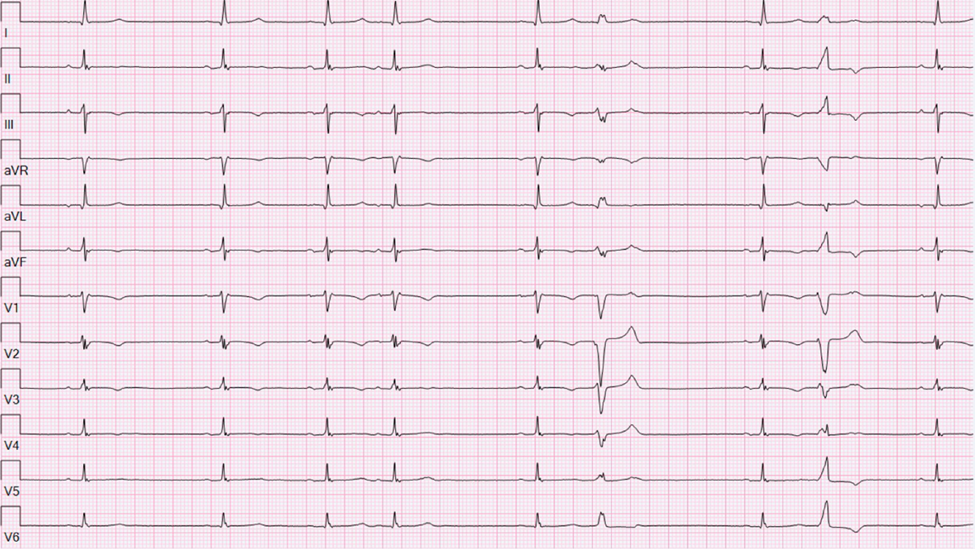
PVC = premature ventricular complex; RV = right ventricular; RVOT = right ventricular outflow tract.
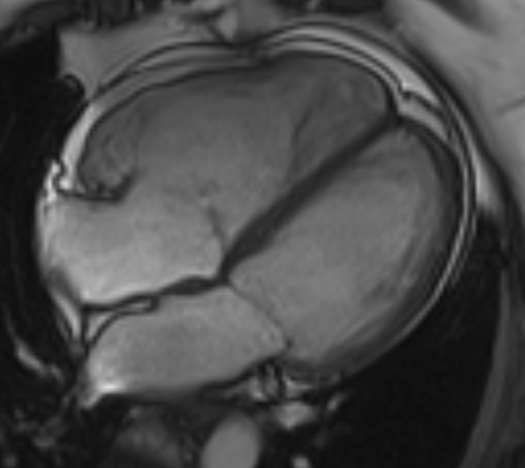
She is next referred for cardiac magnetic resonance imaging (cMRI) and consultation with the Advanced Heart Failure Service because of the RV findings on echocardiogram. A cMRI demonstrates a moderately dilated RV (end-diastolic volume indexed 156 mL/m2; reference range 44-99 mL/m2 per the 2025 Society for Cardiovascular Magnetic Resonance [SCMR] update on Reference Values ["Normal Values"] in cMRI1). RV ejection fraction is reduced at 30% (Video 1). There are also multifocal RV bulging and dyskinesia of the right ventricular outflow tract (RVOT), RV free wall, and inferior wall (Videos 2, 3).
Video 1: 4Ch SSFP Cine Image of the Heart
The RV global systolic function is reduced; RVEF 30%.
4Ch = four-chamber; RV = right ventricle; RVEF = right ventricular ejection fraction; SSFP = steady state free precession.
Video 2: RV Inflow/Outflow SSFP Cine Stack
RVOT dyskinesis.
RV = right ventricle; RVOT = right ventricular outflow tract; SSFP = steady state free precession.
Video 3: Axial Cine SSFP Stack of the Heart
RV inferior wall dyskinesis.
RV = right ventricle; SSFP = steady state free precession.
According to the 2023 European Task Force Criteria for Arrhythmogenic Cardiomyopathy, which one of the following describes the morphologic imaging criteria she met for the most likely diagnosis?
Show Answer