Asymptomatic Wolff-Parkinson-White Pattern in Athletes: Whose Court Is the Ball in?
Quick Takes
- A Wolff-Parkinson-White pattern is a common electrocardiographic finding in screened athletes.
- A structured evaluation can prevent unnecessary restriction and identify athletes truly at risk.
- A multidisciplinary sports cardiology team is recommended to achieve optimal outcomes.
The preparticipation examination (PPE) is an invaluable tool in the care of athletes. Screening electrocardiograms (ECGs), although controversial, are often included in the PPE to improve the sensitivity of identifying cardiac pathology relevant to sudden cardiac arrest (SCA) in athletes. Based on registry data, the Wolff-Parkinson-White pattern (WPWp) is the most common remarkable finding seen on PPE ECGs.1,2
The prevalence of WPWp in the athletic population is approximately 0.1-0.3%, and 0.1% in the general population.3,4 Registries have reported that approximately 1-3% of sudden cardiac death (SCD) cases in athletes are attributed to Wolff-Parkinson-White syndrome (WPWs).3,5 However, this finding may be an underestimate because it is difficult to diagnose WPWs by autopsy and some of these deaths may have been misclassified as sudden unexplained death.3 Therefore, properly assessing and risk stratifying patients with WPWp is of utmost importance in the general athletic population. The athlete presenting with newly diagnosed WPWp on screening PPE should be expeditiously evaluated by a cardiologist familiar with the care of athletes. No recommendations exist as to what type of cardiologist should evaluate these athletes. As the niche of sports cardiology has risen significantly in recent years,6 consideration of a multidisciplinary cardiac evaluation using both a sports cardiologist and sports electrophysiologist is highly recommended (Figure 1).
Figure 1: Foundations of an Athlete Multidisciplinary Cardiac Care Team
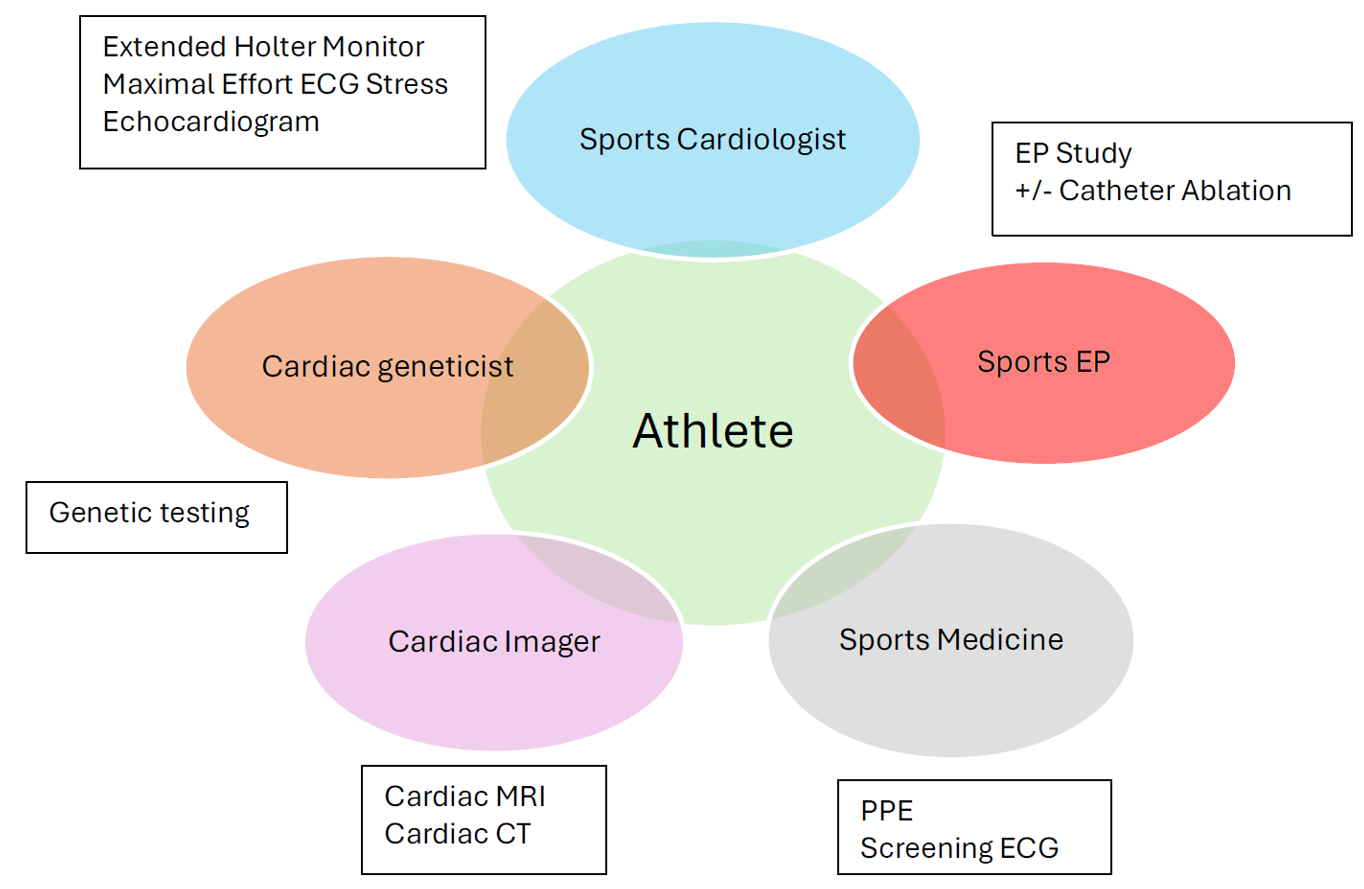
The ideal structure of an athlete multidisciplinary cardiac care team for the evaluation of SCA risk in patients with arrhythmic disorders. The sports cardiologist should initially evaluate these athletes and refer appropriately to other specialized disciplines such as sports EP and cardiac imaging.
CT = computed tomography; ECG = electrocardiogram; EP = electrophysiology; MRI = magnetic resonance imaging; PPE = preparticipation examination; SCA = sudden cardiac arrest.
The first step is determining whether the WPWp is symptomatic; symptoms may include palpitations, syncope, chest pain, dyspnea, cardiac arrest, or supraventricular tachycardia (SVT). For athletes with symptomatic WPWs, upfront electrophysiology study (EPS) and catheter ablation of the accessory pathway(s) being offered are both recommended.1,3 The symptomatic athlete with WPWs should be held from competition and training due to the inherent risk of SCA. The 2024 Heart Rhythm Society (HRS) Expert Consensus Statement on Arrhythmias in the Athlete provides a class 1 recommendation for first-line EPS and catheter ablation if the athlete has WPWs and/or left ventricular systolic dysfunction secondary to ventricular asynchrony.3 The athlete may return to play after successful catheter ablation of the accessory pathway, resolution of symptoms, and close follow-up.
The evaluation and management of athletes with asymptomatic WPWp is less clear given limited evidence. The sports cardiologist can initiate preliminary noninvasive cardiac diagnostic testing to risk stratify the patient's accessory pathway, which should include a maximal-effort ECG stress test,7 transthoracic echocardiogram, and ambulatory ECG monitor to assess durability of the pre-excitation at higher heart rates and any concurrent structural heart disease known to co-exist with WPWs (e.g., Ebstein anomaly, atrial septal defect). In the United States, current guidelines recommend an initial noninvasive assessment of asymptomatic WPWp while allowing the athlete to continue participation in their athletic activity during diagnostic testing.1,3 There is no evidence to suggest that withholding return to play during evaluation increases the asymptomatic athlete's risk of SCD.1 After completion of noninvasive testing, the athlete should be re-evaluated by the cardiac team, which should include a sports cardiologist and sports electrophysiologist.
In the pediatric population, especially in younger patients, symptom reporting is less reliable; malignant arrhythmias in this group correlate more closely with EPS findings than with clinical histories. Therefore, the benefit of proceeding directly to EPS, regardless of noninvasive test results, likely outweighs the risk.3
The role of a sports cardiologist in the evaluation of athletes prior to competition or those with cardiac conditions continues to grow globally. In the case of an athlete with WPWp, the sports cardiologist has a pivotal responsibility in the initial noninvasive assessment of the athlete's accessory pathway SCD risk, evaluation of associated structural heart abnormalities, and evaluation of the physiologic effect of arrhythmic disorder on exercise using a maximal-effort stress test. Lastly, a sports cardiologist can facilitate shared decision-making (SDM) discussions with the athlete, their support system, and organizational stakeholders.
The ideal model recommended by the authors for evaluating an athlete with WPWp should begin with a sports cardiologist. Secondly, the authors recommend the availability of a multidisciplinary cardiology referral system, which must include a sports electrophysiologist at its core. Referral to other cardiac subspecialists such as a cardiac geneticist and/or advanced cardiac imager should be considered for certain individualized cases (Figure 1). Each clinician would provide their own expertise and individual diagnostic workup for the specific condition or risk evaluation. SDM should be implemented by the sports cardiologist and all participating clinicians with the athlete and their support system to determine whether to proceed with an EPS for asymptomatic WPWp.1,3 The role of the sports electrophysiologist is not limited to performing EPS and ablation, but also includes being deeply involved in the SDM process, discussing the risks, benefits, and alternatives of such an invasive approach with the athlete.1,3
Athletes with WPWp who prefer a conservative approach without an EPS should be informed about the importance of an emergency action plan (EAP). All stakeholders—the coaches, athletic trainers, team clinicians, and individual athletes—should be involved in the recognition and prevention of SCA.8,9 The EAP should be a written formalized document that is rehearsed yearly by all members of the athletic team. Members of the team should be trained and certified in cardiopulmonary resuscitation and automated external defibrillator (AED) use.9 AEDs should be readily available within 2-3 min at all training venues.9 Emergency medical services should be properly trained in the treatment of SVT given the nuances of its management in the setting of WPWp and whether it is antidromic or orthodromic atrioventricular re-entrant tachycardia. Special consideration of a personal AED carried by the athlete and/or family member is an option. Data from studies have shown that implementation of an EAP improves response time to SCA in school settings, where time to defibrillation is a critical factor for improved survival and good neurologic outcomes.3
This expert analysis has highlighted the common scenario of an athlete with asymptomatic WPWp on PPE and has recommended a multidisciplinary team led by a sports cardiologist and electrophysiologist (Figure 1). Ensuring safe return to play requires an EAP, and athletes at high risk choosing conservative care may consider a personal AED.
References
- Kim JH, Baggish AL, Levine BD, et al. Clinical considerations for competitive sports participation for athletes with cardiovascular abnormalities: a scientific statement from the American Heart Association and American College of Cardiology. J Am Coll Cardiol. 2025;85(10):1059-1108. doi:10.1016/j.jacc.2024.12.025
- Harmon KG, Zigman M, Drezner JA. The effectiveness of screening history, physical exam, and ECG to detect potentially lethal cardiac disorders in athletes: a systematic review/meta-analysis. J Electrocardiol. 2015;48(3):329-338. doi:10.1016/j.jelectrocard.2015.02.001
- Lampert R, Chung EH, Ackerman MJ, et al. 2024 HRS expert consensus statement on arrhythmias in the athlete: evaluation, treatment, and return to play. Heart Rhythm. 2024;21(10):e151-e252. doi:10.1016/j.hrthm.2024.05.018
- Maclachlan H, Castelletti S, Bhatia R, et al. Prevalence and outcomes of WPW pattern in the young: a report from a nationwide cardiac screening programme (European Journal of Preventive Cardiology website). 2022. Available at: https://academic.oup.com/eurjpc/article/29/Supplement_1/zwac056.280/6583871. Accessed 12/16/2025.
- Finocchiaro G, Westaby J, Sheppard MN, Papadakis M, Sharma S. Sudden cardiac death in young athletes: JACC state-of-the-art review. J Am Coll Cardiol. 2024;83(2):350-370. doi:10.1016/j.jacc.2023.10.032
- Friedman EM, Baggish AL, Chung EH, et al. Sports cardiology as a career pathway: guidance for interested cardiovascular trainees. JACC Adv. Published online October 27, 2025. doi:10.1016/j.jacadv.2025.102305
- Baggish AL, Shah AB. MY APPROACH to the athlete with Wolff-Parkinson-White Syndrome (WPW). Trends Cardiovasc Med. 2018;28(2):154-155. doi:10.1016/j.tcm.2017.09.005
- Martinez M, Kim JH, Friedman EM, Chung EH. Cardiac player health and safety: a call to action. Br J Sports Med. Published online February 20, 2024. doi:10.1136/bjsports-2023-107119
- Friedman EM. How To of Emergency Action Planning (ACC website). 2021. Available at: https://www.acc.org/Latest-in-Cardiology/Articles/2021/09/24/12/05/How-To-of-Emergency-Action-Planning. Accessed 12/16/2025.
Clinical Topics: Arrhythmias and Clinical EP, Congenital Heart Disease and Pediatric Cardiology, Sports and Exercise Cardiology, EP Basic Science, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Congenital Heart Disease, CHD and Pediatrics and Arrhythmias, Sports and Exercise and Congenital Heart Disease and Pediatric Cardiology
Keywords: Sports and Exercise Cardiology, Sports, Death, Sudden, Cardiac, Wolff-Parkinson-White Syndrome, Athletes