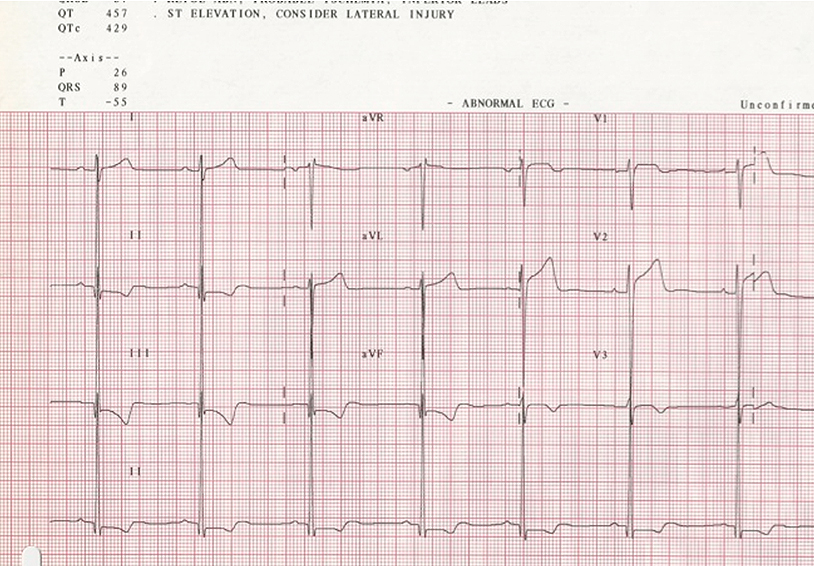
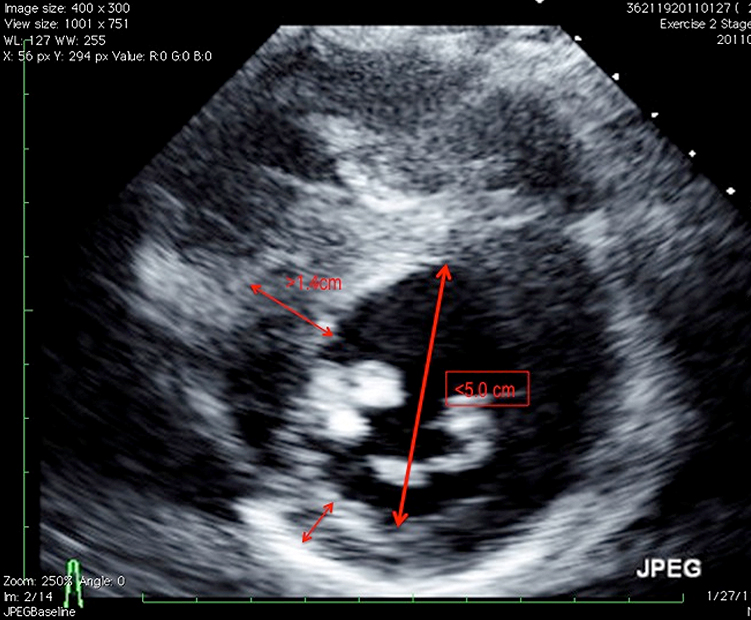
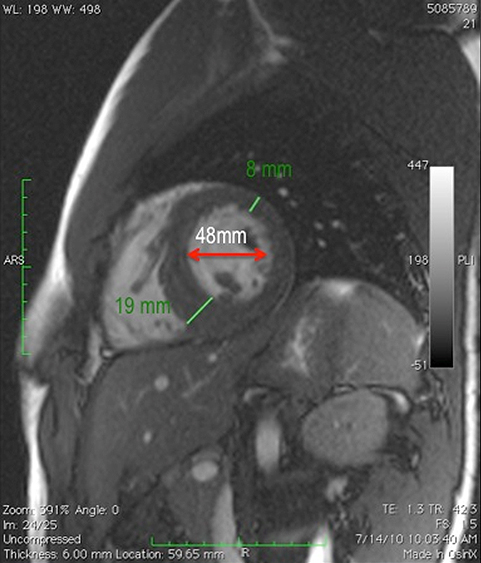
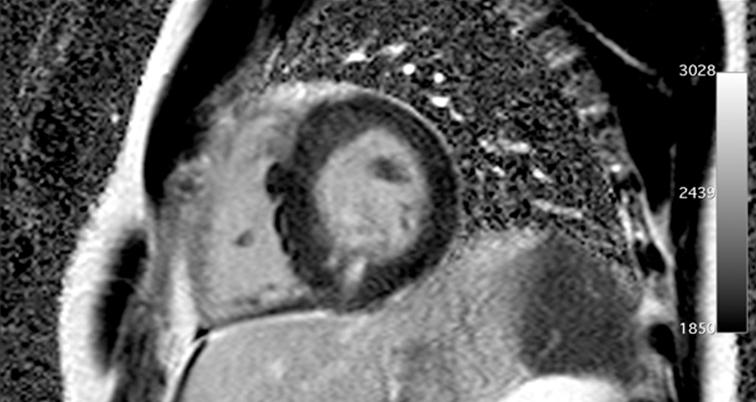
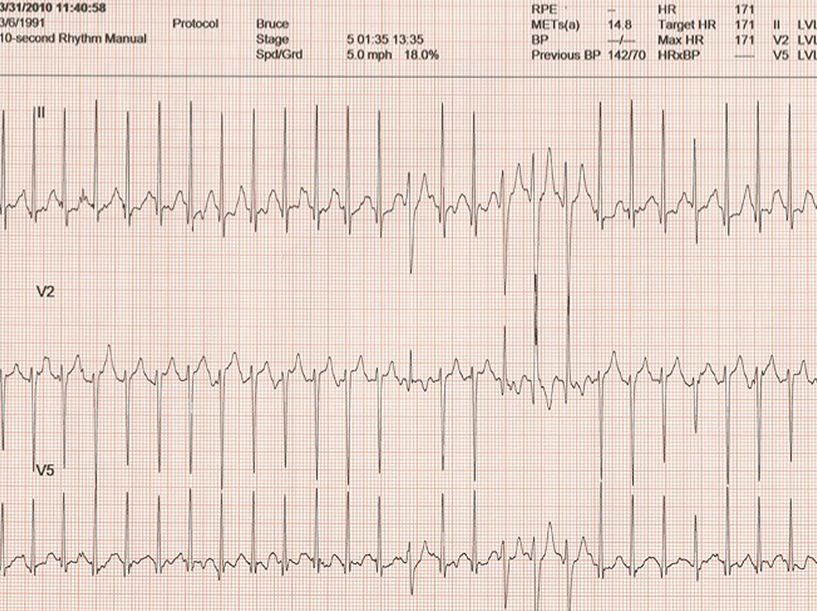
A 19-year-old college athlete with prior diagnoses of a bicuspid aortic valve and an "athletic heart" is scheduled to leave for tryouts for a professional soccer team in Spain. Independent review of his electrocardiogram (ECG) (Figure 1) prompted a closer look at his last evaluation by his pediatric cardiologist. The echocardiogram showed mild AS from a bicuspid valve aortic valve without aortic dilatation (Figures 2 and 3). His left ventricular cavity was small with abnormal papillary muscle size and position (Figure 4). Cardiac magnetic resonance imaging (MRI) was suggested and showed findings similar to the echocardiogram (Video 1); in addition there was delayed enhancement suggestive of fibrosis (Video 2). A stress test was performed, and a 3 beat run of ventricular tachycardia (VT) occurred in stage five (Figure 5). He was restricted from competitive sports and first-degree relatives were evaluated. No gene mutation was identified. His father was screened. Although he had no evidence of aortic valve disease or aneurysm formation, the patient was diagnosed with hypertrophic obstructive cardiomyopathy (HOCM) and was restricted from playing competitive soccer.
Which of the following is the best option for management of this patient?
Show Answer
The correct answer is: G. Start beta blockade therapy, restrict from competitive sports, consider an AICD, and evaluate all first-degree relatives.
Criteria that would exclude this from being labeled as an athletic heart include unusual patterns of left ventricular hypertrophy (LVH) (asymmetric wall thickness), abnormal ECG findings (flipped T waves in inferior leads), family history of HCM, a smaller left ventricular cavity, evidence of scarring on MRI, and VT with exercise. Established guidelines clearly exclude participation in any competitive sports even with prior therapy and an ICD. Recent studies have shown that patients with an ICD can play competitive sports safely but guidelines currently in effect have not yet recognized this. Placement of an ICD in this scenario is less obvious. Risk factors for sudden death present in this patient include an abnormal blood pressure response to exercise and non-sustained VT on stress testing. ICD placement should be considered, but is not absolute. Discussion of risks and benefits of this intervention is necessary so that the patient and his family could develop an informed opinion for possible treatment. Use of beta blockade therapy is a primary treatment of HCM with symptomatic obstruction and ventricular tachycardia. Repeat stress testing in this case may guide adequacy of treatment but should not be used as another chance for sports clearance. The presence of aortic valve disease and HCM together has been reported previously. Careful evaluation of all first-degree relatives is warranted for the possibility of both diseases and all associated complications. Genetic testing may not have a definitive yield.
This case illustrates several valuable points. Clear understanding of screening ECG abnormalities indicative of myocardial disease is essential. Familiarity with standardized criteria (such as the Seattle criteria), though not perfect will improve disease detection and limit false-positive results. The degree of the LVH needs to be proportional to the amount of aortic stenosis. Abnormal patterns of LVH that are not concentric such as varying wall thickness as seen here should trigger further suspicion and testing. The type of sport and conditioning must be taken into consideration when assessing ventricular size and wall thickness. A period of deconditioning followed by repeat evaluation may clarify the diagnosis. The MRI has become routine in the evaluation of HCM. As shown above, MRI confirmed the abnormal echo findings and revealed delayed gadolinium enhancement suggestive of fibrosis. When present independently, these complex pathologies vary both in presentation and expression of disease. Deciphering the etiology becomes more daunting, due to the presence of multiple diseases.
References
Gersh BJ, Maron BJ, Borrow RO, et al. 2011ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines developed in collaboration with the American Association for Thoracic Surgery, American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Failure Society of America, Heart Rhythm Society, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol 2011; 58:e212-60.
Maron BJ. Distinguishing hypertrophic cardiomyopathy from athlete's heart: a clinical problem of increasing magnitude and significance. Heart 2005;91:1380-2.
Feizi O, Farrer Brown G, Emanuel R. Familial study of hypertrophic cardiomyopathy and congenital aortic valve disease. Am J Cardiol 1978;41:956-54.
Maron BJ, Zipes DP, et al. 36th Bethesda Conference: eligibility recommendations for competitive athletes with cardiovascular anomalies. J Am Coll Cardiol 2005; 45:1312-77.
Drezner JA, Ackerman MJ, Anderson J, et al. Electrocardiographic interpretation in Athletes: the Seattle Criteria. Br J Sports Med 2013;47:122-4.