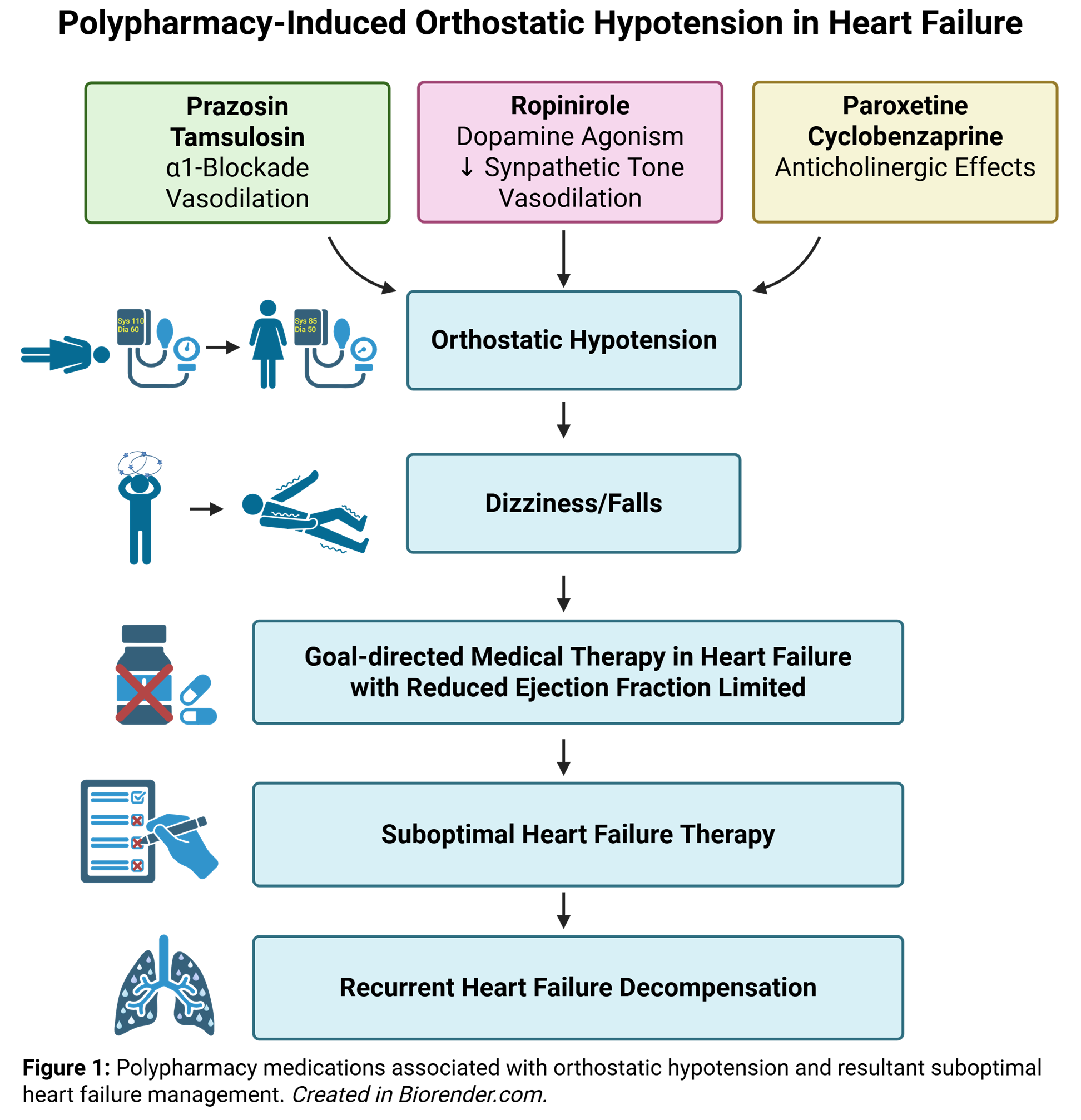
This patient presented with ADHF in the context of suboptimal medical therapy. His ability to tolerate GDMT was limited by orthostatic hypotension (OH), likely exacerbated by polypharmacy. Several of his medications might have contributed to his OH, particularly the anticholinergic effects of paroxetine and cyclobenzaprine, as well as ropinirole (a dopamine D2/D3-agonist) and prazosin (an alpha [α]–1 antagonist). Ropinirole can induce OH mainly through arterial and venous dilation resulting from inhibition of sympathetic nervous system activity. Both prazosin and tamsulosin can result in OH through the vasodilator effect of its α1-adrenergic antagonist properties. The most appropriate next step would be to consult geriatrics medicine for a comprehensive evaluation of polypharmacy, which could facilitate long-term optimization of GDMT by discontinuing one or more medications that contribute to OH.
HF is projected to affect nearly one-half of patients by 2030; patients with HF often present with multiple comorbidities and require complex pharmacological regimens, resulting in significant polypharmacy and sometimes hyperpolypharmacy.1 Polypharmacy, typically defined as the chronic use of five or more medications, remains an underestimated issue in HF management because it contributes to inappropriate prescribing, poor adherence, drug–drug interactions, and adverse outcomes.2 OH is another prevalent and underrecognized condition in older adults, defined as a fall in systolic BP of ≥20 mm Hg or of diastolic BP of ≥10 mm Hg upon standing, with prevalence ranging from 5% to 7% in the general population to approximately 30% in those >65 years of age, and as high as 65% in very old adults. Cardiovascular (CV) contributors of OH include medical treatment for HTN, arrhythmias, coronary artery disease, HF, and sinus node dysfunction, which, when combined with progressive cognitive decline and muscle weakness, can result in increased mortality.3 The prevalence of OH rises with advancing age, mainly because of declining baroreceptor sensitivity and a higher incidence of autonomic neurodegenerative diseases in older adults. The progression and severity of OH in older adults depend largely on associated conditions such as diabetes mellitus or neurodegenerative disorders.4 Additionally, in a systematic review, older adults with frailty were 1.6 times more likely to have OH.5 Pharmacological therapy is a major contributor to iatrogenic OH (Figure 1), with psychoactive and neurologic agents such as tricyclic antidepressants, trazodone, antipsychotics, selective serotonin reuptake inhibitors, benzodiazepines, and antiparkinsonian drugs impairing BP regulation through mechanisms including α-adrenergic blockade, vasodilation, and reduced sympathetic activity, making OH one of the most frequent CV adverse effects of these treatments.6 A subset of these medications also possesses anticholinergic properties, which, when prescribed concurrently, can increase the burden of OH.7,8
Figure 1: Polypharmacy-Induced Orthostatic Hypotension in Heart Failure
Created in BioRender. Le, D. (2026) https://BioRender.com/aavnzx4
Consulting electrophysiology for AF ablation or CRT would not be appropriate in this scenario because he did not have a high AF burden on recent ZioPatch monitoring and did not meet CRT criteria on the basis of his EF and QRSd. Similarly, although digoxin has been shown to reduce rehospitalization in HF, its use would not be appropriate in this case for two reasons. First, its addition would contribute to polypharmacy, and, second, the presence of acute kidney injury would limit its use.
References
- Stefil M, Dixon M, Bahar J, et al. Polypharmacy in older people with heart failure: roles of the geriatrician and pharmacist. Card Fail Rev. 2022;8:e34. Published 2022 Dec 19. doi:10.15420/cfr.2022.14
- Delara M, Murray L, Jafari B, et al. Prevalence and factors associated with polypharmacy: a systematic review and Meta-analysis. BMC Geriatr. 2022;22(1):601. Published 2022 Jul 19. doi:10.1186/s12877-022-03279-x
- Srinivas V, Choubey U, Kapparath S, et al. Age-related orthostatic hypotension: a comprehensive analysis of prevalence, mechanisms, and management in the geriatric population. Cardiol Rev. 2025;33(6):556-566. doi:10.1097/CRD.0000000000000636
- Roca F, Rougette K, Zmuda L, et al. Association between orthostatic blood pressure dysregulation and geriatric syndromes: a cross-sectional study. BMC Geriatr. 2022;22(1):157. Published 2022 Feb 26. doi:10.1186/s12877-022-02844-8
- Debain A, Loosveldt FA, Knoop V, et al. Frail older adults are more likely to have autonomic dysfunction: a systematic review and meta-analysis. Ageing Res Rev. 2023;87:101925. doi:10.1016/j.arr.2023.101925
- Bhanu C, Nimmons D, Petersen I, et al. Drug-induced orthostatic hypotension: a systematic review and meta-analysis of randomised controlled trials. PLoS Med. 2021;18(11):e1003821. Published 2021 Nov 9. doi:10.1371/journal.pmed.1003821
- Wong HL, Weaver C, Marsh L, et al. Polypharmacy and cumulative anticholinergic burden in older adults hospitalized with fall. Aging Med (Milton). 2023;6(2):116-123. Published 2023 Apr 5. doi:10.1002/agm2.12250
- Ilkin Naharci M. Frail older adults with high anticholinergic burden are at risk of orthostatic hypotension. J Am Med Dir Assoc. 2025;26(3):105436. doi:10.1016/j.jamda.2024.105436
