A Mitral Woe, Disordered Flow, the Infant Will Not Grow
A 3-week-old term male neonate with an arcade mitral valve (MV) resulting in mixed MV disease presents to the emergency department with respiratory distress.
His vital signs include heart rate (HR) 151 bpm, respiratory rate 70 breaths/min, blood pressure 93/41 mm Hg, and oxygen saturation 98%. His weight is 4.7 kg (10.4 lbs). Physical examination reveals a diaphoretic infant with suprasternal and intercostal retractions, a grade 3/6 holosystolic murmur at the apex, and hepatomegaly.
An electrocardiogram shows sinus tachycardia, prominent P waves in the left precordial leads, and no ST-segment changes. An echocardiogram is obtained (Image 1).
Image 1
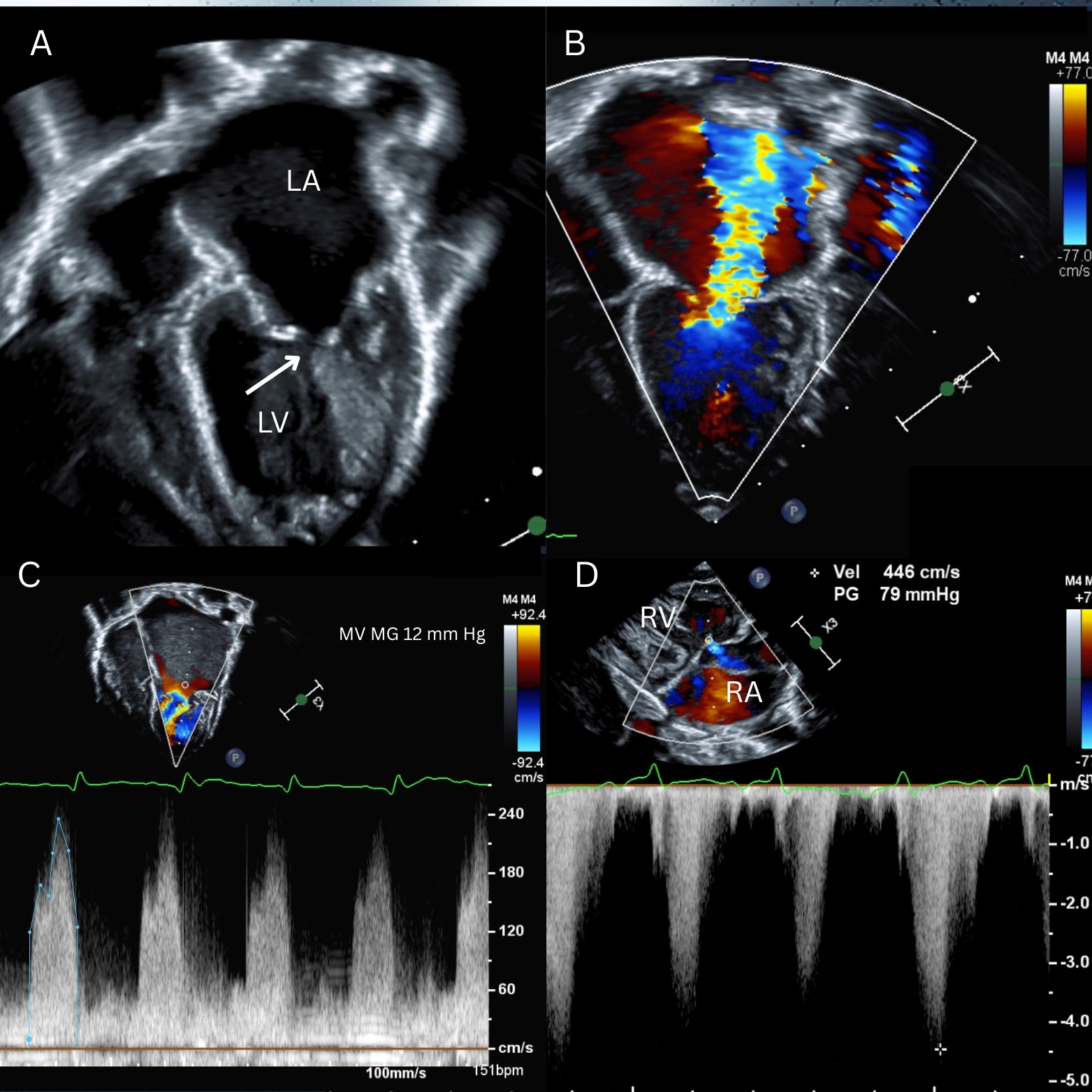
LA = left atrium; LV = left ventricle; MG = mean gradient; MV = mitral valve; PG = peak gradient; RA = right atrium; RV = right ventricle.
Which one of the following would be least helpful in the management of this patient?
Show Answer
The correct answer is: B. Inhaled nitric oxide.
Congenital malformations of the MV can present in the neonatal period with symptoms of pulmonary venous congestion such as increased work of breathing, tachypnea, and failure to thrive secondary to left atrial (LA) hypertension. This patient presented with decompensated heart failure (HF) secondary to significant mitral stenosis (MS) and mitral regurgitation (MR) attributable to an arcade MV. Image 1, panel A (arrow) shows a mitral arcade characterized by elongated papillary muscles connected to each other and to the free edge of the anterior mitral leaflet by a bridge of fibrous tissue as a result of muscularization of the subvalvular apparatus.1 This malformation can lead to MS, MR, or both. This neonate had a severely dilated LA and mildly dilated left ventricle (LV) (Image 1, panel A) with severe MR (Image 1, panel B) and mean gradient 12 mm Hg at resting HR 151 bpm across the MV (Image 1, panel C). In the setting of severe MR, assessment of MS can be challenging because the gradient across the MV can be exaggerated due to increased flow (pulmonary venous flow plus regurgitant volume).
Inhaled nitric oxide is the correct answer because initiation of inhaled nitric oxide would be the least helpful in management of this patient's acute decompensated HF. The elevated right ventricular (RV) systolic pressure of ≥79 mm Hg plus the right atrial pressure is indicative of group 2 pulmonary hypertension (PH; PH secondary to left-sided heart disease), as per the World Health Organization (WHO) classification of PH.2 In the 2022 European Society of Cardiology (ESC) Guidelines for the Management of PH, optimizing treatment of the underlying left-sided heart disease before addressing PH is recommended (class I recommendation, level of evidence A).3,4 Additionally, drugs approved for pulmonary arterial hypertension (PAH) are not recommended in this group. Inhaled nitric oxide is used in the treatment of PAH. It acts by vascular smooth muscle relaxation, decreases pulmonary vascular resistance, and consequently decreases mean pulmonary artery pressure and RV afterload. However, in patients with left-sided obstruction, inhaled nitric oxide can worsen symptoms of pulmonary edema due to its vasodilatory effect. Increased left-sided heart pressure can result in changes in the pulmonary vasculature leading to residual PAH even after the left-sided heart disease is addressed. Postoperative PAH may require treatment with pulmonary vasodilators but should gradually improve with time.
Studies describing the utility of diuretics in pediatric patients with MV disease are limited. Nevertheless, both loop diuretics and thiazides are often employed to decrease pulmonary venous congestion in patients with HF symptoms.5 Although provider practices vary and the evidence is lacking, some have hypothesized that angiotensin-converting enzyme inhibitors and angiotensinogen-receptor blockers can be used in patients with MS and/or MR to reduce LV afterload and improve LV stroke volume.6
Positive pressure ventilation (PPV), specifically positive end-expiratory pressure, reduces LV afterload, LV wall stress, and myocardial oxygen demand. The net effect is improved LV stroke volume. PPV also increases alveolar pressure, improves recruitment and oxygenation, and supports work of breathing.7 These effects reduce pulmonary venous congestion and can be helpful in a neonate with tachypnea and severe MR. Patients with MS can be preload dependent; thus, PPV should be used with caution in these patients due to its preload-reducing effect.
Initial management of congenital MV disease includes optimization of caloric intake to promote weight gain and diuretic therapy to treat pulmonary congestion. Medical management is generally favored for young patients because there is limited availability of MV prostheses small enough for infants and neonates. The definitive management of mitral arcade is primarily surgical and may consist of mitral valvuloplasty, or MV replacement with a bioprosthetic or mechanical valve. MV repair is preferred over replacement in neonates and children because it has lower surgical mortality.8 However, the rate of reintervention and need for eventual MV replacement remain high.8 In some older patients, balloon mitral valvuloplasty can be attempted if congenital MS is the primary concern. In this case, the severe MR limited this option. In the presence of a supravalvular mitral ring, balloon mitral valvuloplasty is less effective and surgical repair is preferred.9
References
- del Nido PJ, Baird C. Congenital mitral valve stenosis: anatomic variants and surgical reconstruction. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2012;15(1):69-74. doi:10.1053/j.pcsu.2012.01.011
- Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S43-S54. doi:10.1016/j.jacc.2009.04.012
- Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618-3731. doi:10.1093/eurheartj/ehac237
- Macera F, Vachiéry JL. Management of pulmonary hypertension in left heart disease. Methodist Debakey Cardiovasc J. 2021;17(2):115-123. Published 2021 Jul 1. doi:10.14797/RKQN5397
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2022;79(17):e263-e421. doi:10.1016/j.jacc.2021.12.012
- Boon NA, Bloomfield P. The medical management of valvar heart disease. Heart. 2002;87(4):395-400. doi:10.1136/heart.87.4.395
- Alviar CL, Miller PE, McAreavey D, et al. Positive pressure ventilation in the cardiac intensive care unit. J Am Coll Cardiol. 2018;72(13):1532-1553. doi:10.1016/j.jacc.2018.06.074
- Bernheim S, Pontailler M, Moiroux-Sahraoui A, et al. Long-term outcomes of infant mitral valve surgery. Cardiol Young. 2025;35(12):2550-2557. doi:10.1017/S1047951125110251
- McElhinney DB, Sherwood MC, Keane JF, del Nido PJ, Almond CS, Lock JE. Current management of severe congenital mitral stenosis: outcomes of transcatheter and surgical therapy in 108 infants and children. Circulation. 2005;112(5):707-714. doi:10.1161/CIRCULATIONAHA.104.500207