A 45-year-old woman who lives alone in a rural area experiences sudden onset of palpitations associated with dyspnea, profuse sweating, paresthesia in both hands, and a rapid pounding sensation in her neck after an argument with a neighbor. She has had similar symptoms for the past several years that usually last <5 min. During one episode, her symptoms resolved after bearing down. Approximately 6 months ago, an episode did not resolve on its own and required her to drive to the local emergency department (ED), approximately 20 min away, where she was found to be in sinus tachycardia. She was advised to follow up with her primary care provider (PCP). At her recent yearly visit with her PCP, she reported these symptoms, noting that her episodes often occur in association with emotional distress and worsen her anxiety. She was prescribed sertraline to treat a panic disorder.
During her current episode, her home blood pressure (BP) device indicates that her BP is 105/76 mm Hg and heart rate (HR) is 145 bpm. She repeatedly tries Valsalva maneuvers, including lying down and raising her legs after straining, with no success. She prepares a large basin full of ice water and submerges her face in it. She shivers but her symptoms persist. She becomes lightheaded and has a sense of impending doom. Frustrated and increasingly anxious, she calls 911, concerned that this episode may be life-threatening.
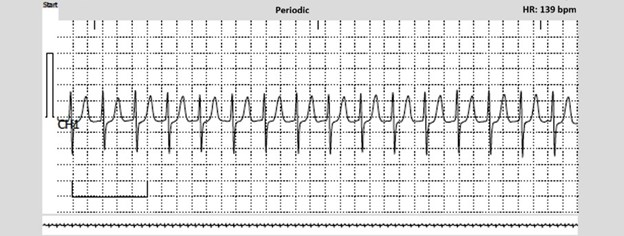
Figure 1
The correct answer is: D. Advise treatment with an oral daily beta-blocker such as metoprolol to treat sinus tachycardia associated with panic attacks and follow-up with her PCP.
The ECG event monitor recording (Figure 1) confirms the suspected diagnosis of PSVT rather than sinus tachycardia. The tracing suggests AVNRT because of the absence of discernible P waves. The evidence base supporting PIP therapy using a beta-blocker or CCB for acute management of PSVT is limited and the available studies only had small numbers of patients. Furthermore, in some cases of PIP therapy, symptomatic hypotension and bradycardia after PSVT termination as well as syncope occurred. The 2015 ACC/American Heart Association/Heart Rhythm Society (ACC/AHA/HRS) Guideline for the Management of Adult Patients With SVT downgraded a PIP management strategy to a Class 2b recommendation, and this strategy was removed from the 2019 European Society of Cardiology (ESC) Guidelines for the Management of Patients With SVT.
Catheter ablation can be curative in >90-95% of PSVT cases and has a Class 1 indication in the current guidelines. However, some patients with PSVT, especially if their episodes are infrequent or not associated with severe symptoms, may prefer to avoid an invasive therapy, its uncommon but potential risks and complications, and its costs. Availability of intranasal etripamil provides a symptom-triggered, on-demand therapy for patients to terminate PSVT episodes outside of a medical setting and represents an additional management option for PSVT other than ablation, chronic suppressive daily therapy, and vagal maneuvers with ED visits as needed. Data from randomized controlled trials of self-administered intranasal etripamil involving almost 2,000 patients with PSVT demonstrated higher and faster conversion rates to sinus rhythm compared with placebo, an acceptable safety and tolerability profile, and a 39% relative risk reduction in ED visits for ongoing PSVT.
This patient case quiz is part of the larger A Modern Look at Paroxysmal Supraventricular Tachycardia (PSVT) grant‑supported initiative, funded by Milestone Pharma. To access additional educational activities on Paroxysmal Supraventricular Tachycardia, please visit the PSVT learning page linked here.
References
- Peng G, Zei PC. Diagnosis and management of paroxysmal supraventricular tachycardia. JAMA. 2024;331(7):601-610. doi:10.1001/jama.2024.0076
- Page RL, Joglar JA, Caldwell MA, et al. 2015 ACC/AHA/HRS guideline for the management of adult patients with supraventricular tachycardia: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. 2016;67(13):e27-e115. doi:10.1016/j.jacc.2015.08.856
- CARDAMYST™ (etripamil) nasal spray. Prescribing information (FDA website). Milestone Pharmaceuticals USA, Inc.; 2025. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/103792s5354lbl.pdf. Accessed 04/10/2026.
- Stambler BS, Camm AJ, Alings M, et al. Self-administered intranasal etripamil using a symptom-prompted, repeat-dose regimen for atrioventricular-nodal-dependent supraventricular tachycardia (RAPID): a multicentre, randomised trial. Lancet. 2023;402(10396):118-128. doi:10.1016/S0140-6736(23)00776-6
- Brugada J, Katritsis DG, Arbelo E, et al. 2019 ESC guidelines for the management of patients with supraventricular tachycardia the Task Force for the Management of Patients With Supraventricular Tachycardia of the European Society of Cardiology (ESC). Eur Heart J. 2020;41(5):655-720. doi:10.1093/eurheartj/ehz467