The P's and Q's Disagree on a Child's ECG
A previously healthy 6-year-old boy presents to the emergency department for treatment of a forearm laceration he sustained while playing in school. He has no history of syncope or recent illness. A detailed cardiac family history has unremarkable findings, including the absence of any autoimmune conditions.
His vital signs include temperature 36.9°C, blood pressure 100/68 mm Hg, respiratory rate 15 breaths/min, and heart rate 40-50 bpm.
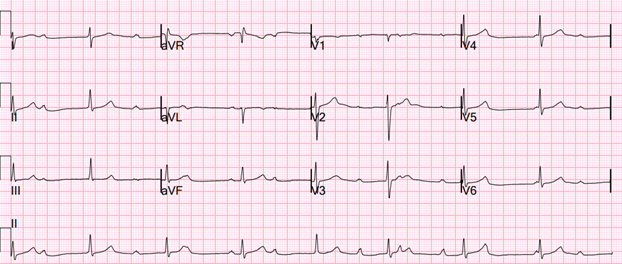
A 12-lead electrocardiogram (ECG) is obtained (Image 1). An echocardiogram demonstrates a structurally normal heart, mild biventricular dilation, normal biventricular systolic function, and normal valvular function.
Image 1: Twelve-Lead Electrocardiogram on Presentation
Which one of the following is the most appropriate next step in his management?
Show Answer
The correct answer is: B. Perform ambulatory cardiac rhythm monitoring.
The most appropriate next step in this patient's management is to perform ambulatory cardiac rhythm monitoring. The 12-lead ECG (Image 1) demonstrated complete or third-degree atrioventricular block (AVB) with a narrow complex junctional escape rhythm. Close examination of the ECG (especially lead II) reveals atrioventricular dissociation, confirming the diagnosis of complete AVB (Figure 1).
Figure 1: ECG Lead II Showing P Waves With a Regular Interval

ECG lead II shows the P waves (red arrows) with a regular interval (lower black arrows) dissociated from the QRS complexes (green arrows), which have a different regular interval (upper black arrows).
ECG = electrocardiogram.
Extended ambulatory rhythm monitoring is now required to determine whether the patient has complex ventricular ectopy, prolonged pauses in ventricular rate, or mean ventricular rate <50 bpm. An ECG only provides a brief sample of the ventricular rate and should not be used as a rate criterion to guide pacemaker implantation.
He might ultimately require permanent pacemaker implantation but did not have an urgent indication on presentation. The 2021 Pediatric and Congenital Electrophysiology Society (PACES) Expert Consensus Statement on the Indications and Management of Cardiovascular Implantable Electronic Devices in Pediatric Patients provides guidelines for the management of isolated complete AVB.1 Class I indications for permanent pacing include: 1) symptomatic bradycardia; 2) wide QRS escape rhythm; 3) complex ventricular ectopy; 4) ventricular dysfunction; and 5) mean ventricular rate ≤50 bpm in infants. Class IIa indications for permanent pacing include: 1) asymptomatic complete AVB beyond the first year of life when the mean ventricular rate is <50 bpm; 2) prolonged pauses in ventricular rate; and 3) left ventricular dilation (z-score ≥3) associated with significant mitral insufficiency or ventricular dysfunction. On the basis of the available data, he did not meet the criteria for permanent pacing.
Neither a cardiac MRI nor an exercise stress test would guide immediate management in this scenario.
In the absence of congenital heart disease and postoperative complete AVB, the etiology of complete AVB in pediatric patients can be categorized into: 1) acquired (including immune mediated); 2) inherited; and 3) idiopathic.2 Immune-mediated AVB can be passively acquired from transplacental passage of the birthing parent's anti-Ro/SSA or anti-La/SSB autoantibodies. Although typically presenting in utero or in the neonate period, AVB may manifest in childhood or even later in adulthood and represents a late progressive congenital form of immune AVB.3 Even though the absence of a family history of autoimmune conditions made this condition unlikely in this patient, testing his birthing parent for autoantibodies would be indicated because it has implications for her future offspring.
Another cause of acquired AVB is infectious myocarditis, with Lyme carditis being a common example.4 The pathogenesis of conduction abnormalities is linked to pathogen tropism for cardiac myocytes and the inflammatory response of the host, and may have an immune-mediated component as well.5 Although this patient did not have any recent illnesses or tick exposure, Lyme titers were obtained and had negative findings.
Inherited AVB is seen in patients with a family history of progressive conduction disease abnormalities. This has been linked to genetic variants in the ion channel genes, including but not limited to sodium voltage-gated channel alpha subunit 5 (SCN5A), sodium voltage-gated channel beta subunit 1 (SCN1B), sodium voltage-gated channel alpha subunit 10 (SCN10A), transient receptor potential cation channel subfamily M member 4 (TRPM4), and lamin A/C (LMNA).6 The absence of a family history of early conduction system disease in this patient made this unlikely.
Idiopathic AVB is diagnosed after exclusion of all common causes of AVB. Idiopathic AVB has been reported during childhood, and its management is guided by the 2021 PACES consensus statement.1 This patient underwent ambulatory cardiac rhythm monitoring, which demonstrated mean ventricular rate 52 bpm and did not reveal complex ventricular ectopy or prolonged/multicycle pauses. He has been closely followed by the pediatric electrophysiology team and, at the time of this writing, has not yet been referred for permanent pacemaker implantation.
References
- Writing Committee Members, Shah MJ, Silka MJ, et al. 2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients: developed in collaboration with and endorsed by the Heart Rhythm Society (HRS), the American College of Cardiology (ACC), the American Heart Association (AHA), and the Association for European Paediatric and Congenital Cardiology (AEPC) endorsed by the Asia Pacific Heart Rhythm Society (APHRS), the Indian Heart Rhythm Society (IHRS), and the Latin American Heart Rhythm Society (LAHRS). JACC Clin Electrophysiol. 2021;7(11):1437-1472. doi:10.1016/j.jacep.2021.07.009
- Baruteau AE, Pass RH, Thambo JB, et al. Congenital and childhood atrioventricular blocks: pathophysiology and contemporary management. Eur J Pediatr. 2016;175(9):1235-1248. doi:10.1007/s00431-016-2748-0
- Lazzerini PE, Capecchi PL, Laghi-Pasini F. Isolated atrioventricular block of unknown origin in adults and anti-Ro/SSA antibodies: clinical evidence, putative mechanisms, and therapeutic implications. Heart Rhythm. 2015;12(2):449-454. doi:10.1016/j.hrthm.2014.10.031
- Charfeddine S, Triki S, Feki W, et al. An unusual cause of a complete heart block in a young healthy man! (a case report). Pan Afr Med J. 2020;37:391. Published 2020 Dec 31. doi:10.11604/pamj.2020.37.391.25927
- Baruteau AE, Probst V, Abriel H. Inherited progressive cardiac conduction disorders. Curr Opin Cardiol. 2015;30(1):33-39. doi:10.1097/HCO.0000000000000134
- Mycinski F, Waldmann V, Kyndt F, et al. Late outcomes of congenital and childhood non-immune, isolated atrioventricular block: a French nationwide retrospective cohort study. Europace. 2025;27(3):euaf040. doi:10.1093/europace/euaf040