Left Ventricular Hypertrophy in Athletes: Elucidating the Gray Zone Through cMRI Tissue Characterization Beyond LGE
Quick Takes
- The gray zone, defined as left ventricular hypertrophy of 1.3-1.5 cm in athletes, represents a significant diagnostic conundrum in sports cardiology with significant management and counseling implications.
- Aside from noninvasive characteristics such as diastolic dysfunction and late gadolinium enhancement, T1 parametric mapping and extracellular volume can be used to distinguish hypertrophic cardiomyopathy (HCM) from athlete's heart due to the presence of cellular disarray and extracellular matrix expansion involved in HCM pathogenesis.
Clinical Vignette
A 19-year-old collegiate volleyball player with no significant medical history was referred for evaluation after she was found to have remarkable electrocardiographic (ECG) findings during a preparticipation screening. She was free of symptoms from a cardiovascular (CV) perspective and carried no family history of cardiomyopathy. Her transthoracic echocardiogram had findings of preserved biventricular function without valvulopathy; however, her left ventricular (LV) basal septal diameter was measured at 1.3 cm.
Combined with her ECG and transthoracic echocardiogram findings of left ventricular hypertrophy (LVH), cardiac magnetic resonance imaging (cMRI) had findings that confirmed basal septal hypertrophy with a measured diameter of 1.3 cm. There was no evidence of late gadolinium enhancement (LGE); however, her T1 mapping time (1,280 msec) and extracellular volume (ECV; 26%) were elevated.
Following the cMRI results, the cardiologist reviewed the findings with the patient and her mother. They asked whether these cMRI findings would impact her ability to continue playing volleyball at a National Collegiate Athletics Association (NCAA) level.
Management Implications of Differentiating Patients in the Gray Zone
Preventing sudden cardiac death (SCD) in athletes is one of the cornerstones of sports cardiology. In a recent study of NCAA collegiate athlete deaths between 2002 and 2022 demonstrating an overall reduction in SCD over the previous few decades, idiopathic LVH/possible cardiomyopathy and hypertrophic cardiomyopathy (HCM) were listed as the second and third most common etiologies of SCD behind autopsy-negative sudden unexplained death.1 The additive risk of intensive exercise in patients with HCM has been a topic of debate, and recent data have suggested no increased risk with the caveat that patients were managed at experienced HCM centers. Thus, the present landscape of sports participation for athletes with HCM has placed emphasis on shared decision-making at centers with high levels of HCM expertise.2 For patients diagnosed with HCM, ensuring appropriate cardiac workup with CV imaging, rhythm monitoring, and screening of first-degree family members are imperative for mitigating risk. With proper diagnosis and risk assessment at experienced centers, it has been demonstrated that athletes can compete at an elite level with low, nonfatal event rates.3
However, it is also important not to assign pathology to normal exercise-induced cardiac remodeling, leading to unnecessary psychological burden on the athlete. It is well known that regular and intensive physical training can cause structural changes to the heart, including increased LV wall thickness and cardiac mass, which contribute to the diagnostic dilemma of differentiating athlete's heart from HCM.4 There is a significant amount of research dedicated to understanding key CV features that can differentiate between these two entities. These may include pathological Q waves, peak oxygen consumption (maximum <50 mL/kg/min), LVH >16 mm, presence of diastolic dysfunction (reduced longitudinal motion—septal E′ velocity <9 cm/sec or E/e′ >15), small LV cavity diameter in end-diastole (<45 mm), or presence of LGE by cMRI.5
Use of T1 and ECV Mapping to Identify Athletes Who Fall in the Gray Zone
The 2024 multisociety Guideline for the Management of HCM endorses the role of cMRI in identifying important differences in the pattern and location of LVH and LV cavity dimensions. The guidelines further describe how the pattern and distribution of LGE can aid in the differentiation of HCM from other CV diseases associated with LVH, including other inherited cardiomyopathies (e.g., lysosomal or glycogen storage diseases), infiltrative cardiomyopathies (amyloidosis), or conditions with secondary hypertrophy attributable to pressure overload (hypertensive heart disease or athletic conditioning).6 Despite these guidelines and parameters, there remains clinical ambiguity regarding how to approach patients in the gray zone—in particular, when clinical variables such as ECG or symptoms suggest pathology but cMRI demonstrates no evidence of LGE.
Using cMRI for tissue characterization has demonstrated relative differences in myocardial composition and has aided in identifying key differences in remodeling that can help differentiate pathology from normal exercise-induced cardiac remodeling. McDiarmid et al. demonstrated myocardial ECV and native T1 in athletes were lower than in untrained control patients (22.5 ± 2.6% vs. 24.5 ± 2.2% [p = 0.02]; 1,178 ± 32 msec vs. 1,202 ± 33 msec [p = 0.02]).7 Although both the cellular and extracellular masses were higher in athletes than in nonathletic control patients (15.8 ± 2.2 vs. 13.6 ± 1.7 [p < 0.001]; 55.1 ± 9.2 vs. 42.3 ± 5.7 [p < 0.001]), the relative expansion of the cellular compartment was greater than the increase seen in the extracellular compartment (130% vs. 116%).7 Taken together, these findings suggest athlete's heart is driven by cellular hypertrophy with a decrease in extracellular expansion. LGE tends to represent a late stage of established fibrosis and has a limited role in detecting the preceding stage of increasing interstitial fibrosis, indicating that perhaps T1 and ECV may be more sensitive and specific.8
Additional studies have examined the role of native T1 and ECV in differentiating HCM from normal structural changes in athlete's heart. These values were found to be lower in athlete's heart than in HCM (1,182 ± 42.4 msec vs. 1,261 ± 66 msec; 22.7 vs. 32.3 ± 7.9%). Furthermore, athletes had significantly lower ECV compared with sedentary control patients (22.7 ± 3.3% vs. 24.3 ± 2.6% [p = 0.006]). The optimal cutoffs used to diagnose HCM were ECV >22.5% (sensitivity 100%; specificity 90%) and native T1 >1,217 msec (sensitivity 81%; specificity 100%). These data, particularly the diverging association of ECV in athletes and HCM, reinforce the belief that an increase in LV mass in healthy myocardium is driven by cellular hypertrophy, whereas, in the setting of HCM, it is mediated by cellular disarray and extracellular matrix expansion. Taken together, T1 and ECV mapping can be used to distinguish athlete's heart from HCM with high diagnostic accuracy (Figure 1).9 This information can help when informing patients about their LVH but, as a single test, remarkable T1 or ECV findings are not enough to give a diagnosis of HCM.
Figure 1: Scatter Plot Showing Maximal Segmental Thickness and ECV of the Same Segment for Patients With HCM and Athletes
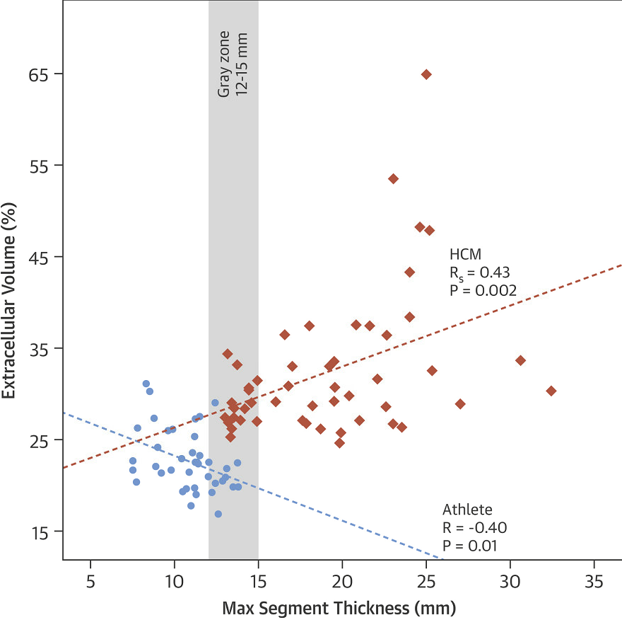
The gray area highlights the indeterminate zone of 12-15 mm.
ECV = extracellular volume; HCM = hypertrophic cardiomyopathy.
References
- Petek BJ, Churchill TW, Moulson N, et al. Sudden cardiac death in National Collegiate Athletic Association athletes: a 20-year study. Circulation 2024;149:80-90.
- Lampert R, Ackerman MJ, Marino BS, et al. Vigorous exercise in patients with hypertrophic cardiomyopathy. JAMA Cardiol 2023;8:595-605.
- Martinez KA, Bos JM, Baggish AL, et al. Return-to-play for elite athletes with genetic heart diseases predisposing to sudden cardiac death. J Am Coll Cardiol 2023;82:661-70.
- Martinez MW, Kim JH, Shah AB, et al. Exercise-induced cardiovascular adaptations and approach to exercise and cardiovascular disease: JACC state-of-the-art review. J Am Coll Cardiol 2021;78:1453-70.
- Martinez MW, Nair SU. The Athlete Grey Zone: Distinguishing Pathologic From Physiologic Left Ventricular Hypertrophy (ACC website). 2014. Available at: https://www.acc.org/latest-in-cardiology/articles/2014/10/14/11/02/the-athlete-grey-zone-distinguishing-pathologic-from-physiologic-left-ventricular-hypertrophy. Accessed 09/11/2024.
- Ommen SR, Ho CY, Asif IM, et al.; Writing Committee Members. 2024 AHA/ACC/AMSSM/HRS/PACES/SCMR guideline for the management of hypertrophic cardiomyopathy: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol 2024;83:2324-405.
- McDiarmid AK, Swoboda PP, Erhayiem B, et al. Athletic cardiac adaptation in males is a consequence of elevated cardiac mass. Circ Cardiovasc Imaging 2016;9:[ePub ahead of print].
- Graham-Brown MP, McCann G. T1 mapping in athletes: a novel tool to differentiate physiological adaptation from pathology? Circ Cardiovasc Imaging 2016;9:[ePub ahead of print].
- Swoboda PP, McDiarmid AK, Erhayiem B, et al. Assessing myocardial extracellular volume by T1 mapping to distinguish hypertrophic cardiomyopathy from athlete's heart. J Am Coll Cardiol 2016;67:2189-90.
Clinical Topics: Noninvasive Imaging, Sports and Exercise Cardiology, Magnetic Resonance Imaging, Sports and Exercise and Imaging
Keywords: Hypertrophy, Left Ventricular, Athletes, Magnetic Resonance Imaging