Feature | Leading With Patients: Elevating Shared Decision-Making Through CardioSmart

Over the last four years, ACC's CardioSmart team has been on a transformative journey – aimed at reshaping how cardiovascular professionals partner with patients in making increasingly complex health care decisions.
As editor, working in close collaboration with ACC's dedicated CardioSmart staff, I had the privilege of growing CardioSmart into a robust and trusted platform – designed to support a new era where shared decision-making (SDM) is not only encouraged, but expected, practiced and resourced.
Our work centered around three main goals: 1) defining and legitimizing SDM across the cardiovascular community; 2) ensuring patients actively guide the development of our tools and research priorities; and 3) fostering the use of decision aids in real-world clinical practice to promote an approach in which informed patient goals and preferences are centered and respected.
We made this progress as a team – clinicians, patients, researchers and staff – united by a commitment to collaborative team-based care and improved heart health for all.
Building On a Strong Foundation
The evolution of CardioSmart has been possible thanks to renowned cardiologists, including the foundational editors Elizabeth Klodas, MD, FACC, JoAnne M. Foody, MD, FACC, and Martha Gulati, MD, MS, FACC, who laid the groundwork for a guideline-driven, patient-centered platform that could grow alongside advances in clinical practice.
Their early investment in creating accessible, evidence-based content designed for patients provided the scaffolding for the innovations in clinician education and patient feedback that we implemented over the last four years.

Driving Real-World Implementation of Decision Aids
Beyond Shared Decision-Making
Although our primary focus was on clinician use of decision aids with patients in practice, we also invested in efforts to meet patients where they are thanks to collaboration between the ACC, clinicians, patients, industry partners and other stakeholders. To date, CardioSmart sponsors and provides content in Higi stations at more than 6,000 commercial pharmacies across the U.S. We built bundles for clinicians to use at community health fairs, and distribute hundreds of free CardioSmart posters for cardiovascular clinics and waiting areas.
Through programs like the Shared Decision-Making Challenge, we also equipped cardiovascular fellows to bring decision aids into their daily encounters. These projects served as training grounds for a new generation of clinicians learning to lead with curiosity, not assumptions, about patient preferences and to use best practices from decades of research in patient engagement.
Our first mission was to move decision aids and infographics beyond publication and into actual practice with a clear value-add to clinicians. The emphasis was that CardioSmart is not just patient education, but a means to patient engagement and empowerment. Use of decision aids at the point of care have been shown to improve patient knowledge, decisional certainty, trust and outcomes,1-4 yet too few are being used at the point of care.
From the beginning, we knew our decision aids would only be effective if they were informed by the lived experiences of patients themselves. We invested heavily in building structured patient forums, feedback loops and co-design processes into everything we developed.
Patient forums focused on diseases like heart failure with preserved ejection fraction; aortic stenosis and tricuspid regurgitation (TR), among others, allowed for direct input and expertise from diverse patients living with the disease. These efforts directly impacted the development of CardioSmart strategy and tools, by identifying areas of confusion, which formats were most helpful, and how to ensure equity across literacy levels, cultural contexts and language access.
This patient-centered model also informed our broader research and quality improvement priorities. For example, we learned that patients wanted more help understanding not just treatments, but how decisions would affect their daily lives and personal goals.
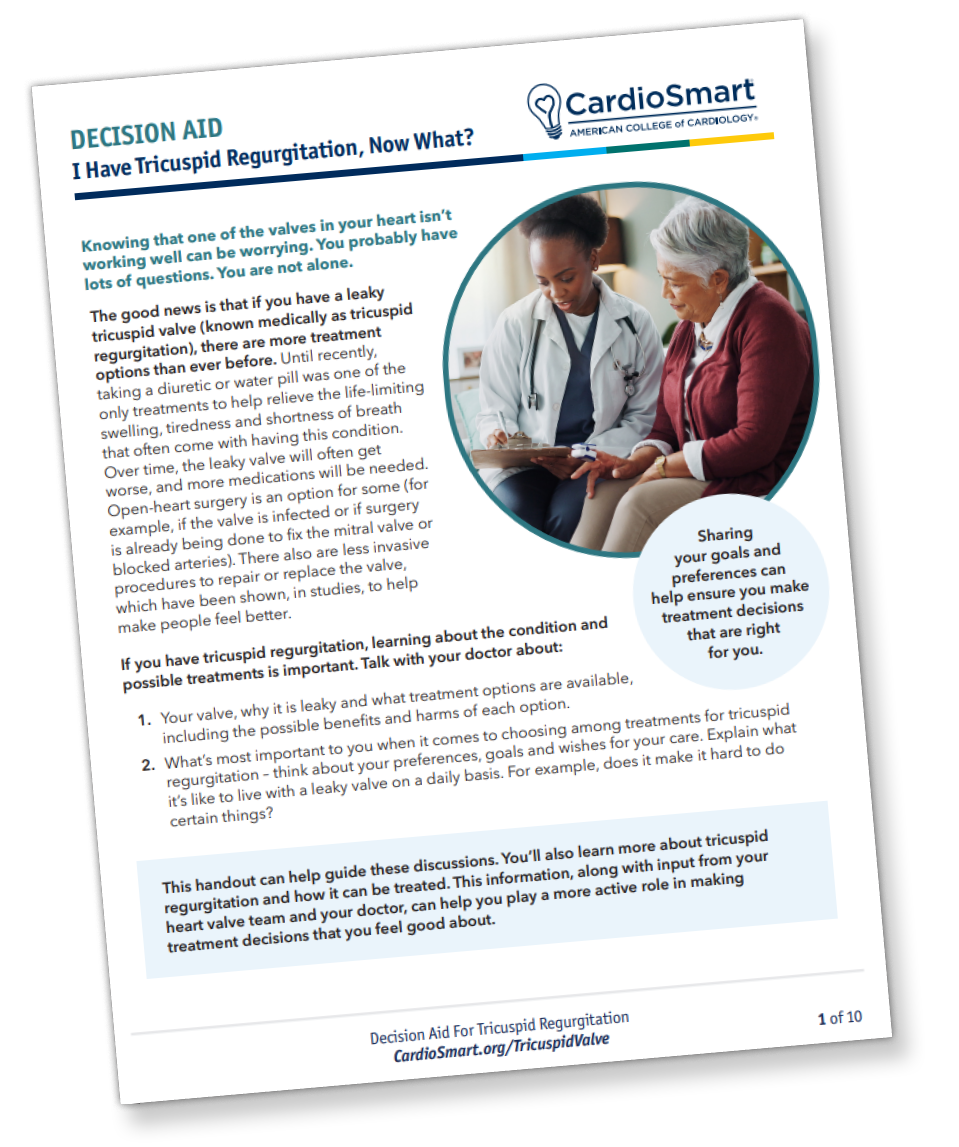
Our work in the CardioSmart TR Hub is one example of this strategy in action, with tools including decision aids, patient education resources and infographics. The voices of the patients were also shared through qualitative research published in JACC: Advances, coinciding with Medicare's National Coverage Determination for transcatheter tricuspid valve repair.5
Legitimizing Shared Decision-Making in CV Care
While implementation was essential, we knew cultural transformation was just as important. SDM had long been referenced in guidelines but rarely operationalized in daily care. We made it a priority to help cardiovascular professionals see SDM not as a "soft skill" but as a clinical imperative – especially for preference-sensitive decisions.
Through CardioSmart, we diligently worked to align our tools and priorities with evolving guideline recommendations. The scope of these efforts required a knowledgeable, passionate team of clinicians. Our assistant editors, comprised of carefully selected practicing cardiologists and fellows across the country, met throughout the year, and in person annually at the ACC Scientific Session, to shape and hone content, and their efforts are greatly appreciated. Today, SDM is a class 1 recommendation across a growing number of cardiovascular guidelines – covering decisions around left atrial appendage occlusion, valve therapies, carotid revascularization and ICD implantation.

Ad hoc groups organized by CardioSmart were also recruited over the past four years to address ongoing requests, including further guidance on defining SDM and clarifying best practices to address the class I recommendations.
These efforts emphasized that SDM is a shared responsibility, across surgeons, interventionalists, general cardiologists, nurses and staff. With increasing coordination across the College, we also ensured our materials were featured when guidelines were disseminated; that decision aids were linked resources to news and coverage on ACC.org and in Cardiology; and shared infographics throughout every annual ACC Scientific Session and other major ACC and cardiovascular society meetings. Even more broadly, CardioSmart decision aids are also part of national research studies testing implementation strategies to encourage use by clinicians in practice.4
Looking Ahead
A foundational value of our work at CardioSmart has been to recognize and elevate the entire cardiovascular care team, including the indispensable contributions of Advanced Practice Clinicians (APCs). Nurse practitioners and physician associates (PAs) are often the most accessible connection patients have in their care journeys. Their communication, education and coordination roles make them essential leaders in SDM.
In recognition of this, I'm thrilled that Viet Le, DMSc, MPAS, PA-C, FACC, is the new editor of CardioSmart, bringing clinical insight, warmth and a steadfast patient focus that reflects the spirit of this platform and the legacy of leadership. I've long believed that term limits are essential to cultivating fresh ideas and ensuring representation, and I look forward to continuing as a passionate mentor, advocate and contributor as Le leads CardioSmart into its next chapter.

CardioSmart's work is far from over. As digital health tools evolve, artificial intelligence expands and care models shift, we have new opportunities – and new responsibilities – to ensure that SDM continues to serve all patients, in all settings.
We will need to remain committed to testing, refining and scaling what works. We must also continue to build partnerships between patients, clinicians and institutions, and keep listening. The best decisions in health care are made together.
Look for exciting updates on healthy living and preparation for upcoming dyslipidemia guideline. There is also a focus on further understanding the goals and preferences for patients with refractory hypertension, as we respond to the proposed Medicare National Coverage Determination for renal denervation, with additional resources to support the hypertension guideline.
I'm deeply grateful to everyone who has joined us on this journey, a team whose unwavering dedication has helped turn CardioSmart into what it is today: a living, evolving model of how we can deliver better cardiovascular care, one conversation at a time.
To explore the latest tools and join this growing community, visit CardioSmart.org.
View a video conversation with Coylewright and Le.
A Collaborative Vision Realized
Looking back, the most remarkable part of this journey is the teamwork and shared leadership that powered it. CardioSmart's evolution was never about one editor or one tool – it was about a movement toward meaningful patient partnership.
Our core CardioSmart team, who met weekly over the past four years, was indispensable in this effort. The team's ability to weave together clinical strategy, technical implementation and organizational priorities gave us the clarity and momentum we needed. This small and mighty team's leadership was steady, thoughtful, and always anchored in the mission of empowering patients and clinicians to make the best decisions together.
As a result of our collective work, CardioSmart now offers:
- Over 1,000 patient education resources and SDM tools across a wide range of cardiovascular conditions
- Multilingual content supporting health equity
- Validated decision aids backed by real-world implementation studies
- Research-aligned content guiding quality improvement efforts
- Strong alignment with ACC/American Heart Association guidelines and policy standards
More importantly, it serves as a platform where patients are not passive recipients of care, but active participants in it and clinicians are guided in the "how to" of implementation of SDM with the use of validated decision aids, as recommended across many ACC guidelines.
This article was authored by Megan Coylewright, MD, MPH, FACC, CardioSmart editor from September 2021 to September 2025.
References
- Stacey D, Lewis KB, Smith M, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev 2024;1(1):CD001431.
- Coylewright M, Otero D, Lindman BR, et al. An interactive, online decision aid assessing patient goals and preferences for treatment of aortic stenosis to support physician-led shared decision-making: Early feasibility pilot study. PLoS One 2024;19(5):e0302378.
- Coylewright M, O'Neill E, Sherman A, et al. The learning curve for shared decision-making in symptomatic aortic stenosis. JAMA Cardiol 2020;5(4):442-8.
- Sepucha K, Elmariah S, Valentine KD, et al. The IMproving treatment decisions for Patients with AortiC stenosis Through Shared Decision Making (IMPACT SDM) Study: study protocol for a cluster randomized stepped wedge trial. Trials 2024;25(1):820.
- Coylewright M, Alston M, Arnold SV, et al. Patient-reported goals in tricuspid regurgitation: A qualitative analysis of patient and care partner perspectives. JACC: Advances 2025;4:101982.
Keywords: Cardiology Magazine, ACC Publications, Decision Support Techniques, Patient Participation