Managing Cardiovascular Disease in Older Adults With Cognitive Impairment: Challenges and Practical Strategies
Quick Takes
- Integrating cognitive function into a cardiovascular (CV) framework can help with guiding polypharmacy, deprescribing support, early capacity assessment, advance care planning, and delirium screening.
- Optimization of the American Heart Association (AHA's) Life's Essential 8 is associated with lower risk of cognitive impairment (CI) and should be prioritized as part of CV prevention in older adults.
- Older adults with CI remain underrepresented in CV trials; therefore, clinical decisions often rely on secondary analyses, observational data, and individualized risk/benefit assessment.
Older adults with cardiovascular (CV) risk factors or established cardiovascular disease (CVD) are at increased risk of cognitive impairment (CI). This risk is observed across several conditions, including hypertension, atrial fibrillation (AF), heart failure, and coronary artery disease.1 Adults with CI and CVD often have coexisting non-CV conditions, including multimorbidity, sarcopenia, frailty, and social isolation, which further complicate their management.
Management may be heterogeneous, with some patients offered a more conservative approach (e.g., lower use of invasive evaluation or revascularization, higher blood pressure [BP] targets, and less intensive low-density lipoprotein cholesterol [LDL-C] lowering), whereas others may receive more intensive treatment despite higher vulnerability to treatment-related adverse events.1 These patterns often reflect personal experience and institutional practice rather than evidence-based approaches, largely because individuals with CI are underrepresented in trials and the available evidence is often limited to secondary analyses.2 Therefore, frameworks that address these challenges holistically may support goal-concordant care, earlier goals-of-care discussions, advance care planning (ACP), palliative care involvement when appropriate, and efforts to reduce caregiver burden and treatment-related adverse events (Figure 1).
Figure 1: Cognitive Impairment in CV Care: A Framework for Individualized Management
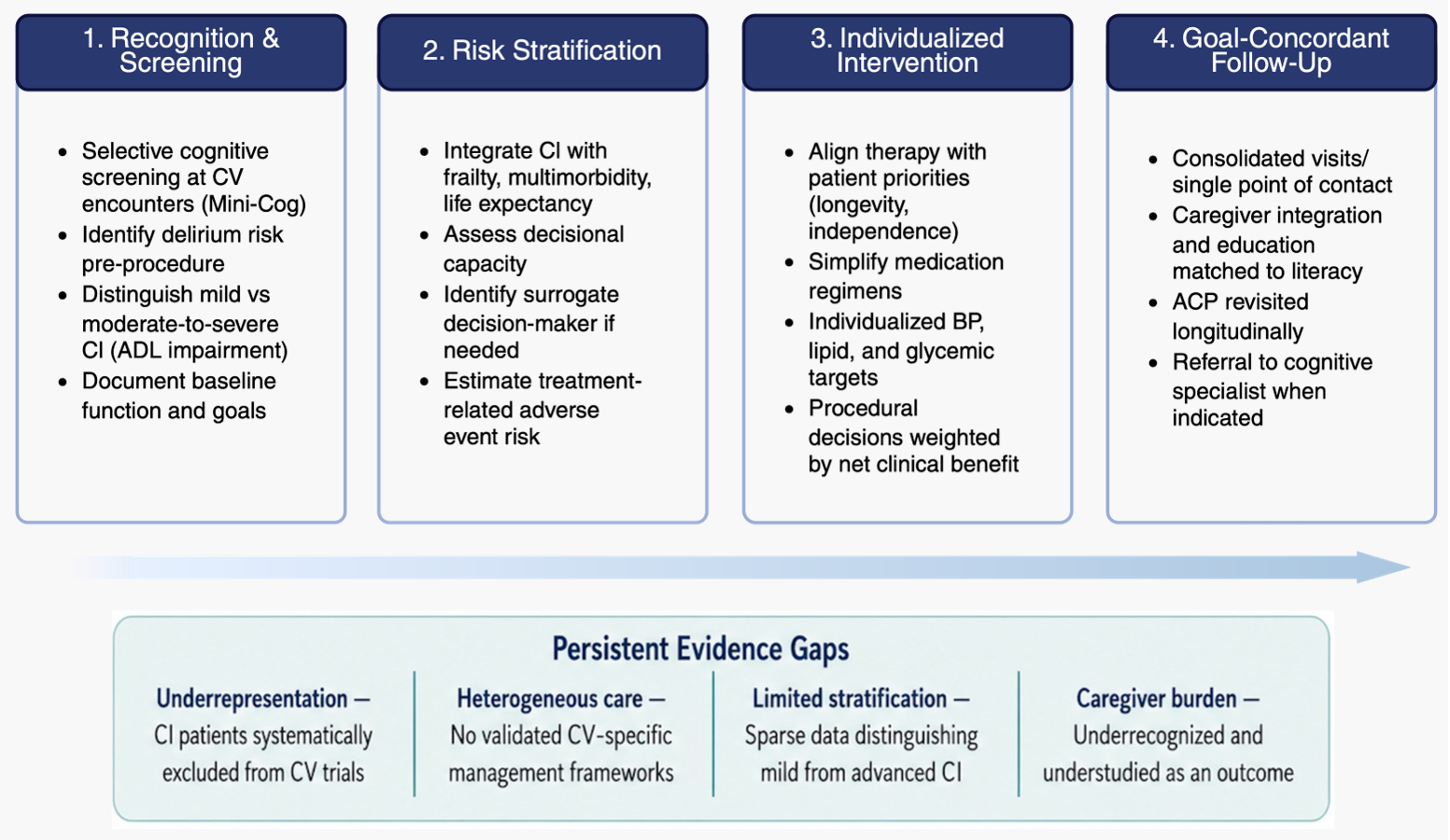
Created in BioRender. Jamil, Y. (2026) https://BioRender.com/76d0gls
ACP = advance care planning; ADL = activities of daily living; BP = blood pressure; CI = cognitive impairment; CV = cardiovascular.
How CI Complicates CVD Management
Challenge 1: reduced self-management and care coordination. Depending on CI severity, recognition of early symptoms (e.g., subtle weight gain, reduced functional capacity, BP fluctuations) may be delayed. Moreover, social and behavioral barriers (e.g., embarrassment and discomfort asking questions) can further delay care.3 Patients with CVD often require multiple visits with various providers, which can complicate their care.
Challenge 2: polypharmacy and medication complexity. Polypharmacy is common in patients with CVD. Among 558 Medicare-insured adults ≥65 years of age hospitalized for HF, 84% at admission and 95% at discharge were prescribed ≥5 medications; 42% of those at admission and 55% at discharge were prescribed ≥10 medications.4 Cardiac regimens frequently require twice-daily dosing, titration, and adverse-effect monitoring, further adding complexity.
Challenge 3: treatment-related adverse events. Individuals with dementia or moderate-to-severe CI may be at higher risk of treatment-related adverse events. For example, among patients undergoing percutaneous coronary interventions, dementia has been associated with higher in-hospital delirium, mortality, kidney injury, falls, and 30-day readmission.5
Challenge 4: informed consent and shared decision-making. Depending on the severity of CI, decisional capacity may be impaired, requiring a surrogate decision-maker. This situation poses challenges when invasive procedures are considered and require shared decision-making.
Challenge 5: underrepresentation in trials. Adults with CI are commonly excluded/underrepresented in CV trials.2 Even when included, cognitive assessment is often limited to a single validated screening tool rather than comprehensive testing. Consequently, treatment decisions are frequently extrapolated from observational data.2
Practical Strategies to Address CI-Related Challenges
- At treatment initiation, clinicians can provide patients with simple, literacy-matched printed instructions on what, how, and when to assess symptoms and potential adverse events.
- Structured telephone support, and caregiver engagement, in addition to consolidated visits and a designated point of contact further reduce fragmentation.
- Routine medication reconciliation may support safer prescribing while prioritizing the use of combination pills, consolidated schedules, caregiver involvement, and deprescribing when appropriate. Available tools include the STOPP/START (Screening Tool of Older Persons' Prescriptions/Screening Tool to Alert to Right Treatment) criteria, Beers criteria, and PRISCUS 2.0 list, along with the use of electronic health records (clinical decision support and alerting for potentially inappropriate medications).6
- Early capacity assessment can be performed with validated instruments such as the MacCAT-T (MacArthur Competence Assessment Tool for Treatment) or the ACE (Aid to Capacity Evaluation), particularly in advanced CI.7
- Early ACP, supported by literacy-matched decision aids and repeated elicitation of goals of care, can be conducted. Tools that can assist include PREPARE (Prepare for Your Care) for YOUR Care (University of California, San Francisco), Five Wishes (Aging with Dignity), and the Serious Illness Conversation Guide (Ariadne Labs).
- Involving geriatrics and palliative care specialists facilitates these conversations and can offer a more comprehensive approach (including care navigation and caregiver support).7
- When a procedure is planned, implementation of nonpharmacologic, multicomponent interventions, such as the AGS CoCare®: HELP (American Geriatrics Society; formerly called Hospital Elder Life Program [HELP]) to reduce delirium risk, may be combined with brief delirium screening tools such as Nu-DESC (Nursing Delirium Screening Scale [NIDUS Measurement and Harmonization Core]), CAM (Confusion Assessment Method), bCAM (Brief Confusion Assessment Method), or the 4AT (Alertness, Abbreviated Mental Test - 4, Attention, Acute Change/Fluctuating Course Assessment Test) to facilitate early identification of delirium.
- Trial-governance strategies may improve protocol inclusiveness. Strategies include avoiding default exclusion, ensuring community engagement and caregiver involvement, using modified consent forms and legally authorized representative pathways, and reducing postenrollment visit burden. Available resources include Duke University Clinical & Translational Science Institute's 5Ts (target population, team, tools, time, tips to accommodate) framework for inclusion of older adults in research, the National Institute on Aging's (NIA's) OutreachPro, and the NIA's ADORE (Alzheimer's and Dementia Outreach, Recruitment, and Engagement) resources for Alzheimer's and dementia trial recruitment and retention.
How CVD Treatment Can Impact Cognitive Function
Assessing and optimizing CV health through the American Heart Association's (AHA's) Life's Essential 8 (LE8) is associated with better cognitive function.1 LE8 includes diet, physical activity, nicotine exposure, sleep, weight management, cholesterol, blood glucose, and BP management. These domains are familiar in cardiology practice and provide a practical framework for cognition and CV health. In the EBBINGHAUS (Evaluating PCSK9 Binding Antibody Influence on Cognitive Health in High Cardiovascular Risk Subjects) study findings, very low LDL-C levels (as low as 35 mg/dL) were not associated with CI over a median of 5.1 years. For select ambulatory adults, the SPRINT MIND (Systolic Blood Pressure Intervention Trial Memory and Cognition in Decreased Hypertension) trial findings support intensive systolic BP lowering to <120 mm Hg for reducing mild CI. However, additional caution is warranted to avoid symptomatic hypotension, orthostasis, falls, and excessive BP lowering. For glucose control, sodium-glucose cotransporter-2 inhibitors and glucagon-like peptide-1 receptor agonists have emerging but unproven cognitive benefits.1
Additional CV-specific considerations are summarized in a state-of-the-art review by Jamil et al.1 In AF, effective stroke prevention and select rhythm-control strategies may reduce cognitive decline, but causal evidence for long-term cognitive benefit remains limited. In patients with AF who also have cerebral amyloid angiopathy or are receiving antiamyloid monoclonal antibodies, anticoagulation decisions may be more complex because of increased cerebral hemorrhage, leaving a potential role for left atrial appendage devices.1 Transcatheter aortic valve implantation is associated with stable or improved cognitive scores, particularly among patients with baseline CI.8 Lastly, carotid artery revascularization has not demonstrated cognitive benefit in asymptomatic individuals, as seen in the CREST-2 (Carotid Revascularization Endarterectomy vs. Stenting Trial 2) findings (the trial compared revascularization with medical management in patients with high-grade asymptomatic carotid artery stenosis).
Future Directions in Managing Adults With CI and CVD
First, dedicated prospective studies without systematic exclusion of adults with CI are needed to identify which older adults with CI are most likely to benefit from specific CV interventions and which are more likely to experience net harm, and to better characterize their cognitive trajectories.
Second, digital cognitive prescreens, predictive models, and digital health platforms may eventually support earlier identification, more aggressive risk-factor optimization, and ACP, but prospective validation is needed.
Third, collaboration with cognitive specialists is needed to develop frameworks for co-management of these individuals to balance benefit and harm.
Fourth, health systems should invest in dedicated CV aging programs such as the model at the Cleveland Clinic, at Mount Sinai, and in Singapore/Asia to develop and test these frameworks.9,10
References
- Jamil Y, Krishnaswami A, Orkaby AR, et al. The impact of cognitive impairment on cardiovascular disease. J Am Coll Cardiol. 2025;85(25):2472-2491. doi:10.1016/j.jacc.2025.04.057
- Anderson TS, Odden MC, Penko J, Kazi DS, Bellows BK, Bibbins-Domingo K. Characteristics of populations excluded from clinical trials supporting intensive blood pressure control guidelines. J Am Heart Assoc. 2021;10(7):e019707. doi:10.1161/JAHA.120.019707
- Lovett RM, Benavente JY, Opsasnick LA, Weiner-Light S, Curtis LM, Wolf MS. Associations between cognitive impairment severity and barriers to healthcare engagement among older adults. J Appl Gerontol. 2023;42(7):1387-1396. doi:10.1177/07334648231166289
- Unlu O, Levitan EB, Reshetnyak E, et al. Polypharmacy in older adults hospitalized for heart failure. Circ Heart Fail. 2020;13(11):e006977. doi:10.1161/CIRCHEARTFAILURE.120.006977
- Kodesh A, Bental T, Vaknin-Assa H, et al. The independent impact of dementia in patients undergoing percutaneous coronary intervention for acute myocardial infarction. Clin Cardiol. 2023;46(3):279-286. doi:10.1002/clc.23967
- Stolfo D, Iacoviello M, Chioncel O, et al. How to handle polypharmacy in heart failure. A clinical consensus statement of the Heart Failure Association of the ESC. Eur J Heart Fail. 2025;27(5):747-759. doi:10.1002/ejhf.3642
- Graven LJ, Kitko L, Abshire Saylor M, et al. Palliative care and advanced cardiovascular disease in adults: not just end-of-life care: a scientific statement from the American Heart Association. Circulation. 2025;151(21):e1030-e1042. doi:10.1161/CIR.0000000000001323
- Pyrpyris N, Dimitriadis K, Papanagiotou P, Tsioufis K. Transcatheter aortic valve implantation and cognitive function: treating the heart, altering the brain?. Struct Heart. 2025;9(9):100695. Published 2025 Aug 5. doi:10.1016/j.shj.2025.100695
- Wong JJ, Chua TSJ, Koh AS. Advancing cardiovascular sciences in ageing for cardiovascular longevity through transformation and implementation. J Asian Pacific Soc Cardiol. 2025;4:e30. doi:10.15420/japsc.2025.15
- Damluji AA, Hashmi AZ, Karthikeyan N, Ancheta OG, Kapadia S, Menon V. Establishing cardiovascular centers on aging: the Cleveland Clinic experience. JACC Adv. 2025;4(12 Pt 1):101987. doi:10.1016/j.jacadv.2025.101987
Clinical Topics: Cardiovascular Care Team, Geriatric Cardiology, Sleep Apnea, Diabetes and Cardiometabolic Disease, Dyslipidemia, Prevention, Stable Ischemic Heart Disease, Valvular Heart Disease
Keywords: Dementia, Cognitive Dysfunction, Geriatrics, Cardiovascular Diseases