Safety of Antiarrhythmic Agents in Breastfeeding Women
Quick Takes
- Use of antiarrhythmic medications in lactating women is necessary to treat maternal cardiac conditions while also allowing for best possible infant outcomes.
- Not all antiarrhythmics are safe with lactation; however, alternative agents may be available within the same drug class.
According to the American Academy of Pediatrics (APA) and the World Health Organization (WHO), exclusive breastfeeding is recommended for the first 6 months of infant life, with continuation up to 2 years or as long as mutually desired by the lactating individual and infant. Beyond its well-documented benefits for infants, lactation also offers significant maternal benefits, including lower lifetime risks of maternal cardiovascular disease and stroke.1 Despite these benefits, the rates of breastfeeding in the United States remain low, reflecting ongoing challenges related to social support, workplace policies, and lactation resources.1,2
For individuals with cardiac conditions, including arrhythmias, lactation presents unique clinical considerations because antiarrhythmic medications must balance maternal cardiovascular stability against minimal infant drug exposure. Medications have a significantly higher risk of transmission to infants via breast milk if they are highly lipophilic or have low serum protein binding. The following are antiarrhythmic drugs for use in lactating women categorized by Vaughan Williams class:
Class I: Flecainide is the preferred rhythm-control agent in lactating patients with structurally normal hearts due to its robust lactation data, with modest infant exposure and minimal or undetectable serum levels.1,3 Propafenone is a suitable Class IC alternative with a comparable safety profile and no reported infant toxicity at standard maternal doses, although pharmacokinetic data are sparser.3 A practical monitoring strategy for both agents includes maternal electrocardiograms (ECGs) to monitor QRS and PR intervals and ≥1 infant ECG in addition to routine pediatric assessments in premature or otherwise high-risk infants.
Quinidine and procainamide are generally considered compatible with breastfeeding, particularly for acute or short-term use with therapeutic monitoring.3 Lidocaine and mexiletine, used primarily for ventricular arrhythmias, are considered reasonable in lactation. Lidocaine's low oral bioavailability in infants makes clinically meaningful exposure unlikely.3,4 Disopyramide is generally avoided because of sparse lactation data, anticholinergic effects, potential milk suppression, and negative inotropy.
Class II: In lactating patients, beta-blockers may be used for acute supraventricular tachyarrhythmias (SVTs), atrial fibrillation, and symptomatic premature atrial or ventricular contractions; milk transfer is inversely proportional to protein binding. Metoprolol, a beta-1 selective inhibitor, is typically the preferred first-line agent due to its high protein-binding properties; if concomitant hypertension is present, propranolol and labetalol are also appropriate. Atenolol, which has low protein binding and is highly excreted in breast milk, should be avoided due to the risk of very high accumulation in infants and potential toxicity.1,5
Propranolol or nadolol are the beta-blockers of choice for patients with primary arrhythmia syndromes like long QT syndrome and catecholaminergic polymorphic ventricular tachycardia or arrhythmogenic cardiomyopathies. Nadolol is highly excreted in breast milk, with a relative infant dose of 4-7%.5 Patients considering pregnancy who are taking nadolol should be evaluated and switched to propranolol during preconception when feasible because high doses of nadolol when lactating pose a significant risk of infant bradycardia.5
Class III: Class III potassium channel blockers display greater lactation safety heterogeneity, warranting a more restrictive approach to their use. Sotalol is the primary option in lactation and can be considered acceptable with caution when Class III therapy is clearly indicated.1 Its low protein-binding properties lead to higher milk transfer and infant exposure, necessitating careful pediatric monitoring for bradycardia, hypoglycemia, and QT prolongation.3 Nonetheless, serious infant adverse events appear uncommon when a structured monitoring plan is in place, supporting its selective use in breastfeeding patients, in whom alternative strategies are inadequate or contraindicated.
Amiodarone is generally avoided due to its long half-life, high lipid solubility, and substantial passage into breast milk, with risks of neonatal thyroid dysfunction, bradycardia, and growth impairment.2,5 American College of Cardiology and Heart Rhythm Society guidelines reserve its use for life-threatening or refractory arrhythmias when alternatives are not feasible, with thorough counseling and pediatric endocrinology involvement.2 Dofetilide, ibutilide, and dronedarone lack lactation data, have narrow therapeutic windows, and carry significant proarrhythmic risk; thus, they should be avoided when alternatives exist.1
Class IV: Verapamil and diltiazem are commonly used across a spectrum of cardiac diseases beyond arrhythmias. Both agents have a large volume of distribution due to their lipophilicity, leading to detectable levels in breast milk. Despite this, the quantity of drug and active metabolite exposure to the infants via milk supply results in quantities <1% of usual infant doses and yields no detectable drug in these infants. As a result, both are classified as compatible with breastfeeding, according to the APA.4,5
Class V: Digoxin is the only cardiac glycoside that has been investigated for use in lactation. It is lipophilic with a large volume of distribution, particularly in infants. Milk:plasma ratios for digoxin are relatively high; however, the relative infant dose via breast milk is approximately 1% of a therapeutic infant dose. Observed infants in case reports showed no clinical signs or symptoms of drug exposure and had undetectable drug levels themselves. The APA has designated digoxin compatible with breastfeeding.4,5
Adenosine, which is produced endogenously by the human body, is also safe to use in lactation for the treatment of acute hemodynamically stable SVT. Patients should be closely monitored for potential adverse effects, including bradycardia, flushing, and dyspnea, all of which typically resolve quickly due to adenosine's short half-life.1,2
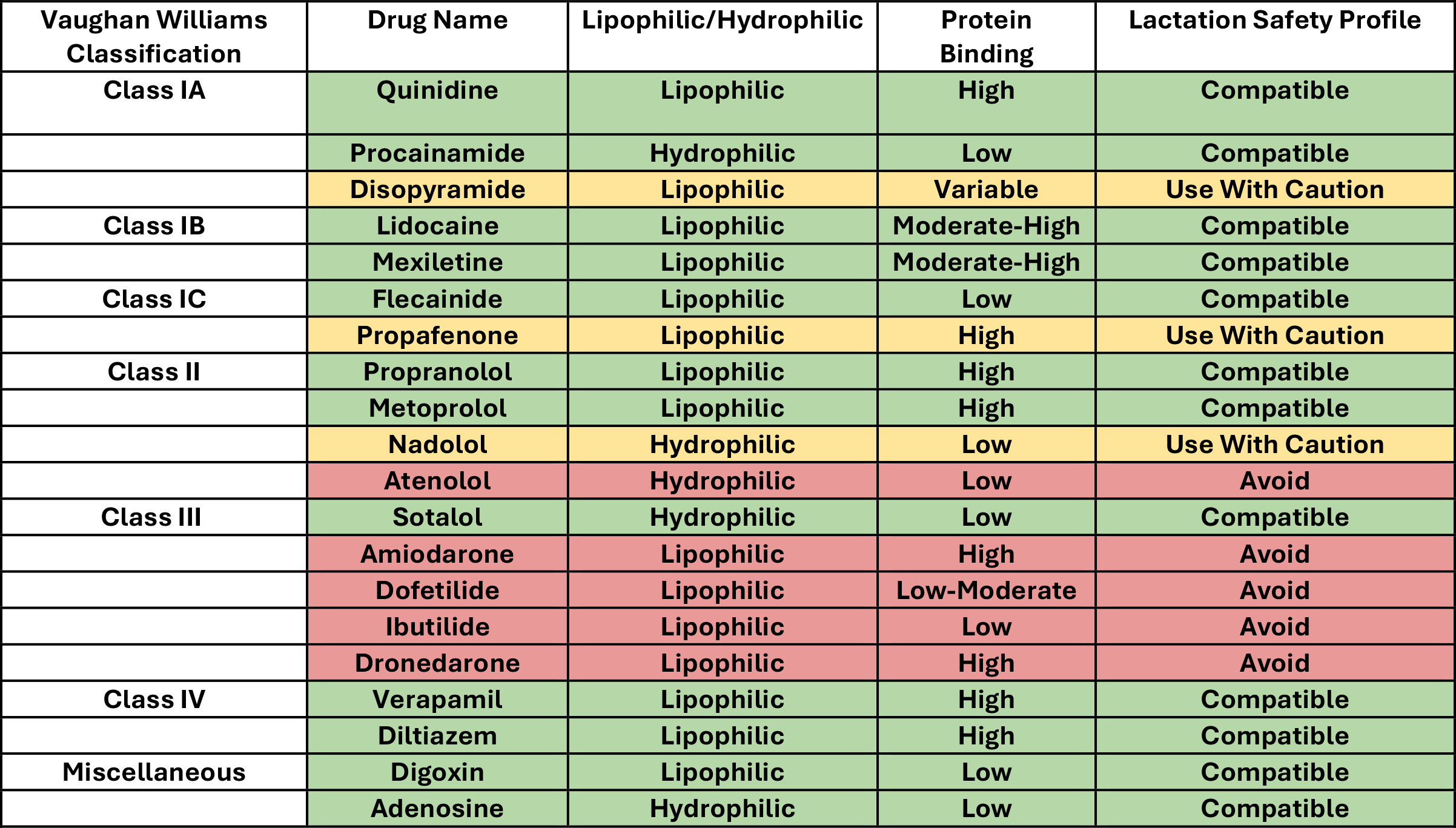
Table 1 summarizes antiarrhythmic drug class properties and their lactation safety profile.
Table 1: Summary of Antiarrhythmic Properties and Lactation Safety Profile
References
- Nunez-Pellot C, Akers A, Običan S, Cain MA, Crousillat DR. Lactation safety of cardiovascular medications. Am Heart J Plus. 2025;55:100552. Published 2025 May 8. doi:10.1016/j.ahjo.2025.100552
- Joglar JA, Kapa S, Saarel EV, et al. 2023 HRS expert consensus statement on the management of arrhythmias during pregnancy. Heart Rhythm. 2023;20(10):e175-e264. doi:10.1016/j.hrthm.2023.05.017
- National Institute of Child Health and Human Development. Drugs and Lactation Database (LactMed®) (National Library of Medicine website). Available at: https://www.ncbi.nlm.nih.gov/books/NBK501922/. Accessed 06/15/2026.
- Briggs GG, Towers CV, Forinash AB. Briggs Drugs in Pregnancy and Lactation: A Reference Guide to Fetal and Neonatal Risk, 12th ed. Lippincott Williams & Wilkins; 2022.
- De Backer J, Haugaa KH, Hasselberg NE, et al. 2025 ESC guidelines for the management of cardiovascular disease and pregnancy. Eur Heart J. 2025;46(43):4462-4568. doi:10.1093/eurheartj/ehaf193
Clinical Topics: Arrhythmias and Clinical EP, Implantable Devices, EP Basic Science, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias, Prevention, Cardiovascular Care Team
Keywords: Cardio-Obstetrics, Arrhythmias, Cardiac, Breast Feeding, Lactation, Anti-Arrhythmia Agents