Nanosecond PFA Demonstrates Safety, Efficacy at 1 Year For PAF
Nanosecond pulsed field ablation (nsPFA) demonstrated reasonable safety, good lesion durability and favorable one-year clinical effectiveness in patients with symptomatic paroxysmal atrial fibrillation (PAF), according to a first-in-human study presented at HRS 2026 and simultaneously published in JACC: Clinical Electrophysiology.
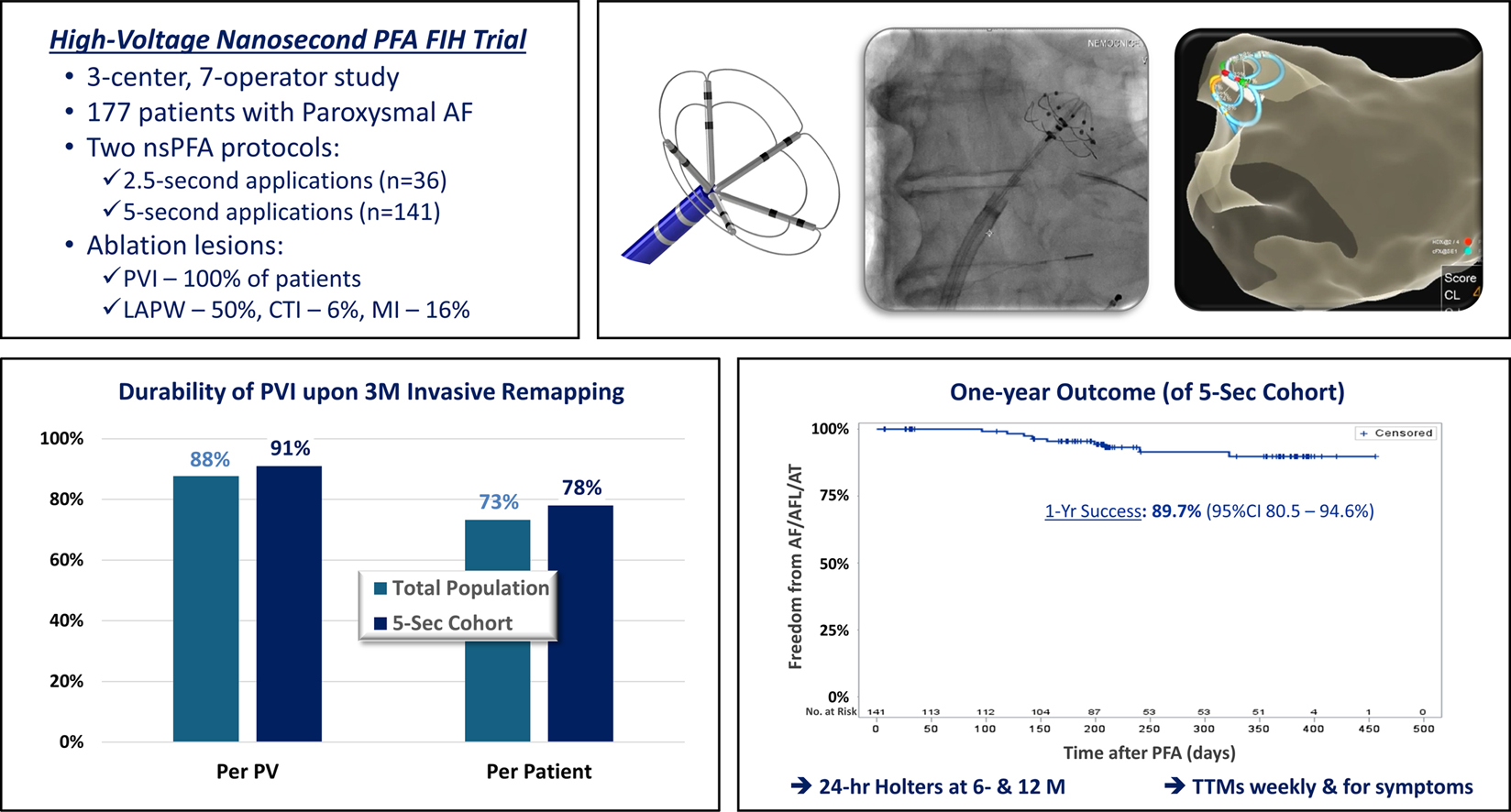
In the prospective, single-arm, open-label trial conducted across three European centers, 177 patients with PAF (mean age, 61; 36% women; mean left atrium diameter, 41 mm) underwent pulmonary vein isolation (PVI) using either a 2.5-second (n=36) or five-second (n=141) protocol with a novel circular nsPFA catheter.
Procedures were efficient, with an average total procedure time of 61.1 minutes, including a short ablation time (mean, 12.6 minutes for PVI), low fluoroscopy exposure (mean, 8.7 minutes) and a mean left atrial catheter dwell time of 19 minutes.
Additional ablation was needed in some patients at the left atrial posterior wall (LAPW; n=87; 49.0%), mitral isthmus (n=29; 16.4%) and cavotricuspid isthmus (CTI; n=11; 6.2%). For PVI, LAPW, mitral isthmus and CTI, the average number of PFA applications per patient were 12.6, 4.6, 2.4 and 3.2, respectively.
Results showed that using the nsPFA catheter alone, acute electrical isolation of all PVs, the primary effectiveness endpoint, as well as LAPW isolation and bidirectional block of the mitral isthmus or CTI, was achieved in all cases.
At invasive remapping, performed at a mean of 13.8 weeks in 139 patients, durable PVI was observed in 87.7% of PVs (478/545) overall, and all PVs were durably isolated in 73.4% of patients (102/139). Efficacy improved to 90.8% of PVs and all veins isolated in 77.7% of patients with the five-second protocol.
At one year, freedom from recurrent atrial fibrillation/atrial flutter/atrial tachycardia was observed in 86.5% of all patients and 89.7% of the five-second cohort.
Overall serious adverse event rate was 1.7%, with three patients experiencing inflammatory pericardial effusion, hemolysis with acute kidney injury and stroke. In a substudy of 35 patients who had a screening brain MRI, an 11.4% rate of silent cerebral events and 11.4% of silent cerebral lesions was observed. There were no cases of esophageal injury, phrenic nerve palsy, PV stenosis or death.
"It is well accepted that achieving durable PVI is essential for enhancing long-term freedom from atrial arrhythmia recurrence," write study investigators Vivek Y. Reddy, MD; Jan Petru, MD; and colleagues. "With the nsPFA catheter, we observed good PVI durability, both acutely and at [three]-month invasive remapping, particularly when using [five]-second pulses. This favorable durability likely stems from the inherent biophysical advantages of nanosecond PF waveforms."
Clinical Topics: Arrhythmias and Clinical EP, Implantable Devices, SCD/Ventricular Arrhythmias, Atrial Fibrillation/Supraventricular Arrhythmias
Keywords: Pulmonary Veins, Atrial Fibrillation, Catheters, Electrophysiology
< Back to Listings