FASTR: Reprieve System Safely Accelerates Decongestion in Acute HF
The Reprieve System, a three-part approach to diuretic therapy, safely produced significantly faster decongestion in patients with acute heart failure (HF) compared with optimal diuretic therapy (ODT), according to results of the FASTR trial published May 4 in JACC: Heart Failure.
Investigators James E. Udelson, MD, FACC, and colleagues randomized 96 patients who had been hospitalized with acute-on-chronic HF with estimated ≥10 lbs. fluid overload and chronic loop diuretic use ≥30 days (mean age, 63 years; 45% women; median baseline estimated glomerular filtration rate, 49 mL/min/1.73m2; excess fluid volume, 20 lbs.) to either ODT (n=44) or the Reprieve System (n=52) of individualized, real-time diuretic response monitoring, automated dosing/titration of intravenous furosemide based on diuretic response and personalized sodium chloride replacement.
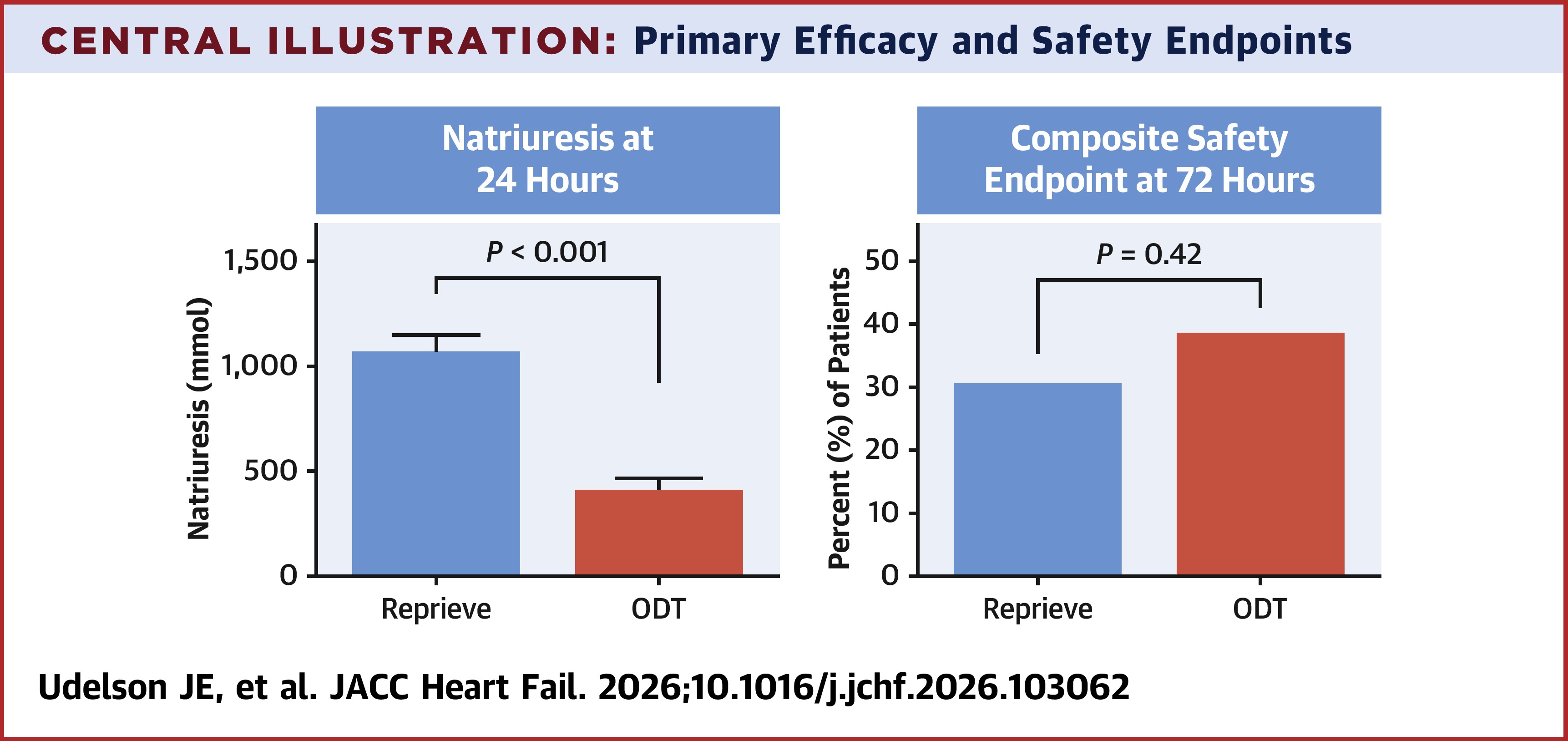
Results showed that 24-hour natriuresis was significantly higher with the Reprieve System compared with ODT (1,082 vs. 423 mmol; p<0.001), while 31% of the Reprieve group vs. 39% of the ODT group experienced the primary safety endpoint – a composite of dialysis or doubling creatinine levels, severe electrolyte abnormalities, hypotension or hypertensive emergency. There were no significant differences in length of stay or 90-day death or HF hospitalization between the two groups.
Additionally, intravenous diuretic therapy duration was shorter (46 hours vs. 88 hours; p=0.014), and rate of weight loss, net fluid loss and net natriuresis were all significantly faster with Reprieve, with little change in serum creatinine levels (0.19 vs. 0.31 mg/dL; p=0.07) between the two groups.
"By continuously quantifying urine output and intermittently measuring sodium excretion, the system targets the most relevant physiological endpoint in [acute HF] – natriuresis – and translates it into real-time therapeutic adjustments," write Wilfried Mullens, MD, PhD; Marnicq van Es, MD; and Sankar D. Navaneethan, MD; in an accompanying editorial comment. "This directly addresses one of the central weaknesses of current care: delayed and often inadequate titration of diuretics."
"Rapidly and safely treating congestion remains an obligatory task in the care of patients with [acute HF]," write the trial investigators. "Hospitalized patients with [acute HF] are highly symptomatic, often medically unstable, and most will remain so until decongestion occurs. Faster decongestion could enable earlier discharge or repurpose hospital time toward other diagnostic (e.g., amyloid cardiomyopathy evaluation, valve replacement work-up, ischemic evaluation) and therapeutic (e.g., GDMT titration, cardioversion, revascularization) activities, which are generally deferred until volume status is improved."
Clinical Topics: Cardiovascular Care Team, Heart Failure and Cardiomyopathies, Acute Heart Failure
Keywords: Renal Dialysis, Natriuresis, Heart Failure
< Back to Listings