First-Ever Guideline Addresses CKM Syndrome
The new 2026 AHA/ACC/ADA/ASN Guideline for the Prevention, Detection, Evaluation, and Management of Cardiovascular-Kidney-Metabolic (CKM) Syndrome is the first ever to address the "interrelated condition characterized by the interconnections among metabolic risk factors (including obesity and type 2 diabetes), chronic kidney disease (CKD) and cardiovascular disease." The document retires, replaces and expands upon the 2013 Guideline for the Management of Overweight and Obesity in Adults. Read the full guideline in JACC.
The guideline outlines the four stages of CKM syndrome and reviews risk factors, including excess weight, high blood pressure, abnormal lipids, high blood glucose and reduced kidney function. It also provides comprehensive recommendations for screening, prevention and treatment that range from healthy lifestyle behaviors to medications and/or metabolic and bariatric surgery.
"Heart, kidney, and metabolic conditions don't occur in isolation – they are deeply connected," said Chiadi E. Ndumele, MD, PhD, MHS, chair of the guideline writing committee. "This guideline calls for earlier screening and care, focusing on prevention and coordinated action to reduce the risk of cardiovascular disease before serious complications develop or a major cardiac event occurs."
Top Takeaways
Key guideline recommendations include:
- Improved risk assessment using new PREVENT equations to estimate 10- and 30-year risk for cardiovascular disease. These equations take into account kidney and metabolic health factors for a more comprehensive and precise estimation of risk compared with previous tools. (Read a new ACC/AHA Scientific Statement outlining the rationale for using the PREVENT equations.)
- Screening for social drivers of health, including food insecurity, housing instability and financial strain.
- Coordinated interdisciplinary care that involves a CKM coordination point person to facilitate patient-centered care and adherence to guidelines.
- Reinforcement of healthy lifestyle behaviors, including physical activity, nutrition, weight, blood pressure, blood sugar and cholesterol. Taking action early can make a meaningful difference in overall health, according to the authors.
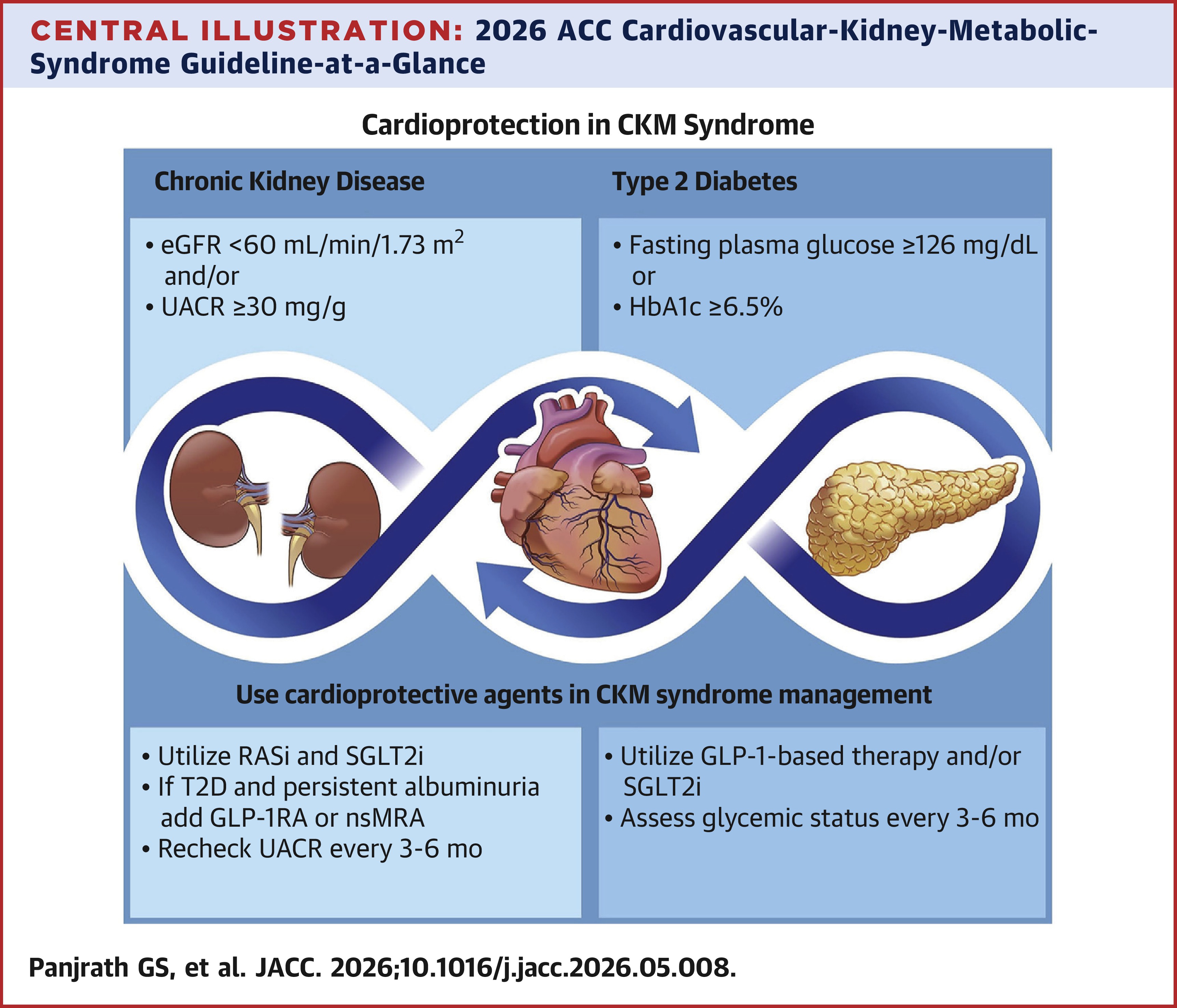
- Additional treatment options that include medications and surgical therapies in conjunction with lifestyle management to manage blood pressure, cholesterol, blood sugar, weight and to protect the heart and kidneys. For the first time, GLP-1-based therapies are recommended for select individuals with obesity and/or type 2 diabetes, and other cardiovascular risk factors. The guideline also recommends use of both estimated glomerular filtration rate (eGFR) and urine albumin-to-creatinine ratio (UACR) "to characterize CKD and guide the use of kidney-protective agents to confer both cardiovascular and kidney benefits."
Looking Ahead
Going forward, the authors note that some unanswered questions still remain, particularly for CKM syndrome patients with heart failure. They also highlight the lack of data to inform the treatment of patients with both heart failure and CKD, as well as those with advanced CKD. Additionally, they say it will be important to relook at education and training, as well as structural factors like automated technology, billing and reimbursement policies, communication, shared clinical space, etc. in order to optimally implement guideline recommendations to meet the needs of various clinical and geographic settings.
The guideline, led by the AHA and ACC, was developed in collaboration with and endorsed by the American Diabetes Association; the American Diabetes Association Obesity Association; and the American Society of Nephrology. It was also published in Circulation.
New Scientific Statement
A corresponding AHA/ACC Scientific Statement on the Use of Predicted Risk and Expected Benefit to Guide Decision-Making in [CKM] Syndrome for the Primary Prevention of Cardiovascular Disease, was also published in JACC. According to Writing Group Chair Sadiya S. Khan, MD, MSC, FACC, et al., the statement "reviews and synthesizes" the evidence supporting the new Guideline's recommendations for the use of predicted risk "to inform staging, strategies for efficient detection of subclinical [cardiovascular disease] in appropriate patients, and decision-making for CKM therapies to support uptake and implementation."
They add that the statement "also offers practical guidance for applying risk assessment as the first step in shared decision-making and for addressing gaps in awareness, risk communication, and optimal implementation."
Clinical Topics: Cardiovascular Care Team, Diabetes and Cardiometabolic Disease, Dyslipidemia, Heart Failure and Cardiomyopathies, Prevention, Lipid Metabolism, Nonstatins, Acute Heart Failure, Exercise, Hypertension
Keywords: Glucagon-Like Peptide 1, Lipids, Heart Failure, Obesity, Kidney, Cholesterol, Bariatric Surgery, Primary Prevention, Patient-Centered Care, Hypertension, Exercise, Glomerular Filtration Rate, Diabetes Mellitus, Type 2, Renal Insufficiency, Chronic, Blood Glucose, Blood Pressure, Creatinine