Mechanical Leaflet Splitting is Feasible in High-Risk Patients Undergoing Valve-in-Valve TAVR
Mechanical leaflet splitting in patients with anatomically high-risk undergoing valve-in-valve (ViV) TAVR saw high procedural success, according to a study published June 25 in JACC: Cardiovascular Interventions.
Raj R. Makkar, MD, FACC, et al., included 150 patients (mean age 79 years, 60% female) from 28 centers undergoing ViV TAVR for either failed surgical (63%) or failed transcatheter valves (37%) from February to November 2025. These patients were determined to have elevated risk by preprocedural CT, and both procedural and safety outcomes were assessed.
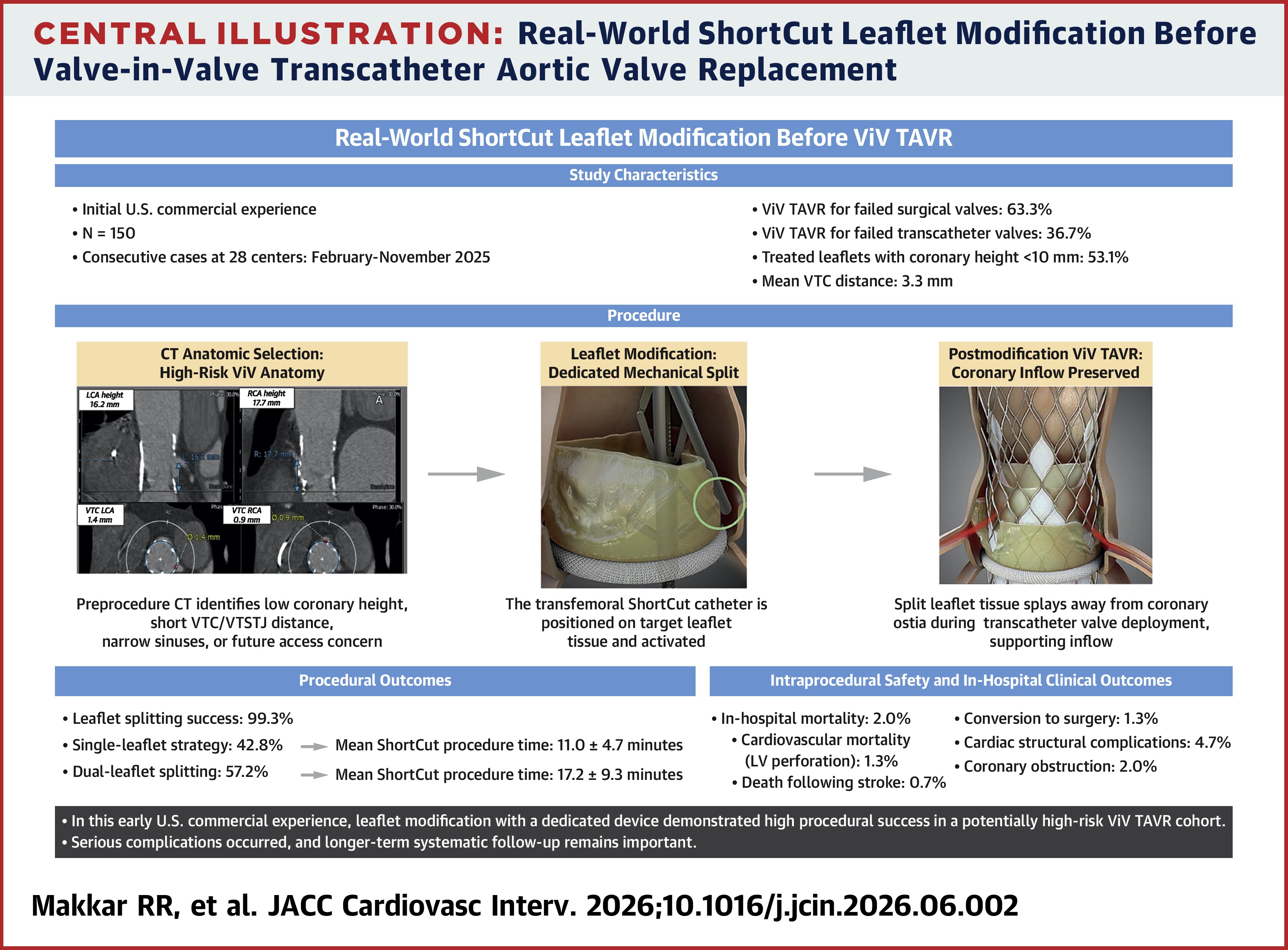
In 87% of patients, CT analysis predicted risk of acute coronary obstruction. Combined risk of sinus sequestration and direct ostial obstruction was observed in 51%. Among the 145 patients where leaflet splitting was attempted, 99% saw procedural success. Dual-leaflet splitting occurred in 57% of the cohort.
Serious complications did occur, with 2% suffering from coronary obstruction and 2% from all-cause mortality. Two deaths were from left ventricular perforation, and one was following stroke. In addition, 1.3% of patients experienced conversion to surgery.
"These findings suggest that dedicated mechanical leaflet modification in a contemporary U.S. real-world practice is feasible and facilitates ViV TAVR in a cohort that is at high risk of coronary obstruction," write the authors. "...Longer-term prospective follow-up with independent adjudication is now needed. In particular, future studies should evaluate delayed coronary obstruction, coronary reaccess, valve performance and redo-TAVR-specific outcomes."
Clinical Topics: Cardiac Surgery, Invasive Cardiovascular Angiography and Intervention, Noninvasive Imaging, Interventions and Imaging, Computed Tomography, Nuclear Imaging
Keywords: Transcatheter Aortic Valve Replacement, Tomography, X-Ray Computed