A 17-Year-Old Soccer Player With Mosaic Turner Syndrome on Growth Hormone With a Bicuspid Aortic Valve, Mild AS, and Aortic Dilation | Patient Case Quiz
A 17-year-old female with mosaic Turner syndrome (TS) on growth hormone (GH) therapy has a history of a bicuspid aortic valve and mild aortic stenosis (AS). She presents for her annual cardiac clearance for sports participation. She has been followed for several years with trending of her aortic measurements and aortic valve gradient. She is a competitive soccer player and plays on several travel teams. She plans to play competitively in college. She is otherwise healthy and feels well. She is followed by cardiology and endocrinology regularly.
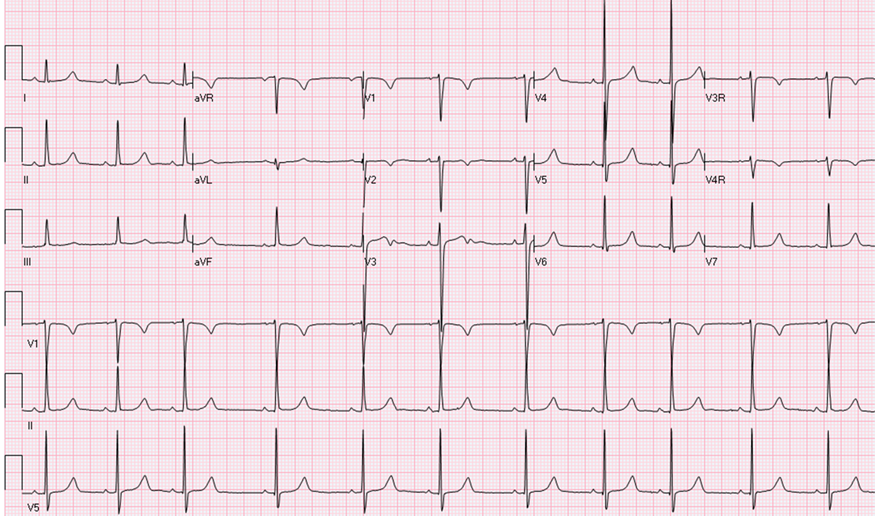
At her clinical evaluation her height is in the third percentile and weight is in the 10-25th percentile on an uncorrected growth curve. Her resting heart rate (HR) is 68 bpm and blood pressure is 107/72 mm Hg in her right arm and 119/57 mm Hg in her right leg. Her cardiac exam reveals a regular rate and rhythm, normal S1 and S2. A click is heard at the right upper sternal border (RUSB). She has a II/VI systolic ejection murmur at the RUSB and left upper sternal border (LUSB) with no radiation to her back. The remainder of her physical exam is normal. Her electrocardiogram (ECG) is shown (Figure 1). Her echocardiogram shows normal biventricular function, a functional bicuspid aortic valve with mild flow acceleration on color Doppler and a peak systolic gradient of 29 mm Hg (mean gradient of 16 mm Hg) across the aortic valve. There is no left ventricular (LV) hypertrophy, and the LV mass is normal. Her aortic root measurements by echocardiogram are shown below (Table 1). She underwent cardiovascular magnetic resonance imaging (MRI), which revealed normal ventricular volumes (LV mass indexed of 62.8 gm/m2, Z score 1.5). Her aortic measurements on magnetic resonance angiography (MRA) showed an aortic root of 2.6 x 3.0 cm and an ascending aorta of 3.0 x 3.2 cm. She also underwent a progressive exercise test on a treadmill using the Bruce protocol showing her to have a VO2 max of 43.5 mL/kg/min. at peak exercise (124% of predicted) and peak respiratory exchange ratio (RER) of 1.03. Her HR and blood pressure responded appropriately to exercise.
Which of the following is the best management course for this patient?
Show Answer
The correct answer is: E. Answers A or D are both correct.
This case has several learning points. TS, a fairly common chromosomal abnormality that affects females, occurs with the complete or partial absence of one sex chromosome. It affects approximately one out of 2,000 live female births.1 The phenotype consists of short stature and ovarian failure. Arguably the most clinically significant feature is congenital heart disease, occurring in approximately 1/3 of patients. The most common cardiac abnormalities are left sided obstructive lesions, such as bicuspid aortic valve, AS, and coarctation.2 Patients with TS have known connective tissue abnormalities and are known to be at risk for aortic dilation. The cystic medial necrosis seen in Marfan syndrome has been reported in TS patients.3 Aortic dissection accounts for 2-3% of deaths in all patients with TS.4,5 Aortic dissection or rupture may occur in relatively young individuals regardless of the presence of a bicuspid aortic valve, suggesting that the vasculopathy alone predisposes these patients to aortic root dilation and aortic dissection. Regular cardiology screening is recommended for all patients with a diagnosis of TS. Exercise restrictions in patients with TS are based upon their cardiac diagnosis.
The factors that may limit this patient from competition are her aortic valve disease and her aortic root dilation. Our patient has mild AS for which the current recommendations are that she can participate in all competitive sports given her normal ECG, normal exercise tolerance, and absence of symptoms. Of concern is the presence of aortic root dilation in the context of systemic disorder that causes a known vasculopathy. While her baseline aortic dilation is less than the 40 mm recommendations in the current Bethesda guidelines, one may argue that her ascending aortic size is certainly above the 95th percentile when matched for her BSA (Z score of 5.4). If one chooses the adult guidelines, one could recommend participation in all competitive sports. Those following her as an adolescent who has not achieved full stature could argue that she should be restricted from high static and high dynamic competitive sports.4 In this particular case, there may be no right answer (between A and D), but her cardiologist chose to allow her to participate in soccer competitively.
Discontinuation of GH therapy would not be indicated. Therapy with exogenous recombinant GH is now routinely used for short stature in TS.2 The disorders of GH excess and dysregulation of the GH/insulin-like growth factor-I (IGF-I) axis can directly cause cardiac hypertrophy and cardiomyopathy.7 With use of exogenous GH, there is a subsequent association with increased LV mass and stroke volume.8 However, GH therapy, specifically in girls with TS, has not been shown to have an effect on either LV morphology or size of the ascending aorta.9 Despite enlargement of her aortic root, there is no strict cardiac indication for exercise restriction.
References
Ranke MB, Saenger P. Turner's syndrome. Lancet 2001;358:309-14.
Bondy CA. Care of girls and women with turner syndrome: a guideline of the turner syndrome study group. J Clin Endocrinol Metab 2007;92:10-25.
Lin AE, Lippe BM, Geffner ME, et al. Aortic dilation, dissection, and rupture in patients with turner syndrome. J Pediatr 1986;109:820-6.
Price WH, Clayton JF, Collyer S, De Mey R, Wilson J. Mortality ratios, life expectancy, and causes of death in patients with turner's syndrome. J Epidemiol Community Health 1986;40:97-102.
Schoemaker MJ, Swerdlow AJ, Higgins CD, Wright AF, Jacobs PA, United Kingdom Clinical Cytogenetics G. Mortality in women with turner syndrome in great britain: a national cohort study. J Clin Endocrinol Metab 2008;93:4735-42.
Bonow RO, Cheitlin MD, Crawford MH, Douglas PS. Task force 3: Valvular heart disease. J Am Coll Cardiol 2005;45:1334-40.
Colao A, Vitale G, Pivonello R, Ciccarelli A, Di Somma C, Lombardi G. The heart: an end-organ of gh action. Eur J Endocrinol 2004;151:S93-101.
Maison P, Chanson P. Cardiac effects of growth hormone in adults with growth hormone deficiency: A meta-analysis. Circulation 2003;108:2648-52.
Bondy CA, Van PL, Bakalov VK, Ho VB. Growth hormone treatment and aortic dimensions in turner syndrome. J Clin Endocrinol Metab 2006;91:1785-8.