A 61-year-old man with history of persistent atrial fibrillation, hyperlipidemia, obstructive sleep apnea and hypothyroidism presented to our outpatient clinic with recurrent lower extremity edema 14 months after atrial fibrillation ablation. One week following ablation he had developed left shoulder pain and shortness of breath. Echocardiogram revealed pericardial and pleural effusions and he was treated with colchicine, celecoxib and furosemide. Several months later he developed leg and abdominal swelling and was started on prednisone 40 mg twice daily tapered over two months, but symptoms persisted. Medications at the time of the visit were notable for rivaroxaban, furosemide and armour thyroid. Physical examination revealed jugular venous distension with Kussmaul's sign, regular cardiac rate and rhythm with a pericardial knock, a distended abdomen and moderate edema of the bilateral lower extremities. Electrocardiogram showed normal sinus rhythm with borderline low voltage (Figure 1). Laboratory evaluation was notable for normal markers of inflammation (high sensitivity C-reactive protein 1.5 mg/L and erythrocyte sedimentation rate 2 mm/hr). Transthoracic echocardiogram revealed a prominent diastolic bounce and respirophasic shift of the interventricular septum, a dilated and non-collapsible inferior vena cava and mitral annular medial e' greater than lateral e' (Figure 2). Cardiac magnetic resonance imaging (MRI) on presentation showed mild pericardial thickening (3mm), no pericardial effusion, no pericardial delayed gadolinium enhancement and a prominent respirophasic shift (Figure 3). Right heart catheterization revealed the following pressures: right atrium 13 mmHg, right ventricle 32/14 mmHg, pulmonary artery 34/20 mmHg (mean 25 mmHg), pulmonary capillary wedge pressure 22 mmHg, left ventricular end-diastolic pressure 20 mmHg; there was respiratory discordance between the right and left ventricles, with systolic area index of 1.53 (Figure 4).
Figure 1
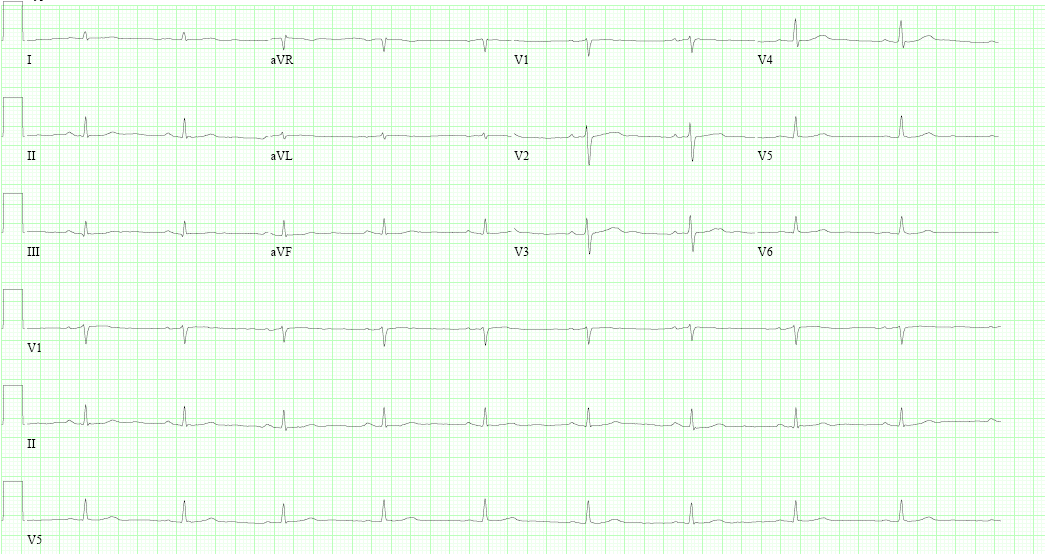
Figure 1: Electrocardiogram.
Figure 2
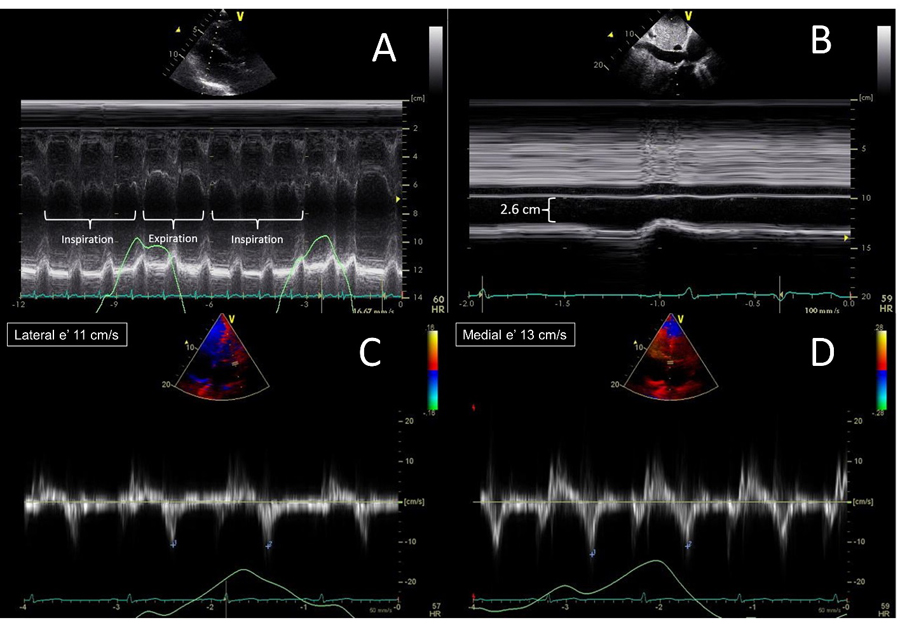
Figure 2: Transthoracic echocardiogram. M-mode across the interventricular septum in the parasternal long axis view showed the diastolic bounce and respirophasic shift (Panel A). The inferior vena cava was plethoric and non-collapsible (Panel B). Tissue Doppler of the mitral annulus in the apical 4-chamber view shows that medial e' was greater than lateral e' (Panels C and D).
Figure 3
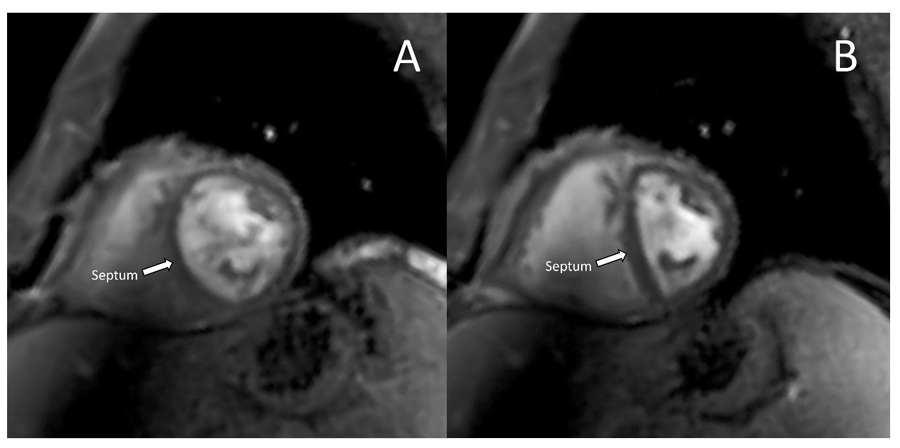
Figure 3: Cardiac magnetic resonance imaging showed mild pericardial thickening (3mm), no pericardial effusion, no pericardial delayed gadolinium enhancement and a prominent respirophasic shift (red arrow). Panel A shows normal septal position during expiration; Panel B shows the septum shifted to the left during inspiration.
Figure 4
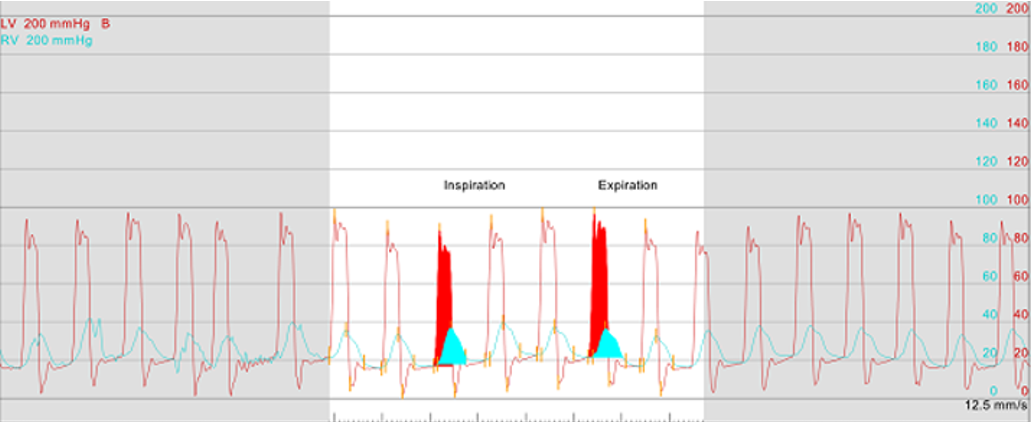
Figure 4: Simultaneous left and right ventricular pressure tracings show end-diastolic equalization of pressures and discordance between the left and right ventricles with inspiration.
Which of the following is the best next step in management of this patient?
Show Answer
The correct answer is: D. Refer for radical pericardiectomy.
This patient developed constrictive pericarditis after atrial fibrillation (AF) ablation. The disease has been refractory to medical therapy and there is no longer evidence of active inflammation, so he should be referred for pericardiectomy (answer D). Constrictive pericarditis is a known complication of electrophysiology ablation procedures, although its exact incidence is unknown.1 A meta-analysis of 192 studies including 83,236 patients undergoing catheter ablation for AF did not report the incidence of constrictive pericarditis, but did report a 1.0% rate of cardiac tamponade and 0.7% rate of pericardial effusion, conditions which can trigger the inflammatory process leading to constriction.2 Smaller studies designed specifically to look for pericardial effusions immediately post-ablation have reported a higher incidence (13-22%) although most of these effusions are small and asymptomatic.3-5
Radical pericardiectomy is the mainstay of treatment for chronic pericarditis. Medical therapy of a few months duration with anti-inflammatory drugs may reverse transient pericardial constriction in 10-20% of patients, but this approach has already failed in our patient.6,7 Cardiac MRI and laboratory testing can help identify patients with constrictive pericarditis likely to respond to medical therapy. In one series of 29 patients, those with increased pericardial thickness, more pericardial late gadolinium enhancement and elevated C-reactive protein and erythrocyte sedimentation rate were more likely to have reversible constrictive pericarditis than those without these characteristics.8 Because our patient presented with more than one year of symptoms, no significant elevation in markers of inflammation, and no late gadolinium enhancement of the pericardium on MRI, the likelihood of responding to medical therapy was very low, so he was referred for pericardiectomy. He underwent successful pericardiectomy and several months later had returned to an active lifestyle, hiking and skiing regularly.
References
Ahsan SY, Moon JC, Hayward MP, Chow AW, Lambiase PD. Constrictive pericarditis after catheter ablation for atrial fibrillation. Circulation 2008;118:e834-5.
Gupta A, Perera T, Ganesan A, et al. Complications of catheter ablation of atrial fibrillation: a systematic review. Circ Arrhythm Electrophysiol 2013;6:1082-8.
Chierchia GB, Capulzini L, Droogmans S, et al. Pericardial effusion in atrial fibrillation ablation: a comparison between cryoballoon and radiofrequency pulmonary vein isolation. Europace 2010;12:337-41.
Lellouche N, Sebag FA, Elbaz N, et al. Acute pericardial effusion following atrial fibrillation ablation: characteristics and relationship with arrhythmia recurrences. Arch Cardiovasc Dis 2011;104:450-7.
Schaer BA, Maurer A, Sticherling C, Buser PT, Osswald S. Routine echocardiography after radiofrequency ablation: to flog a dead horse? Europace 2009;11:155-7.
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Cremer PC, Kumar A, Kontzias A, et al. Complicated pericarditis: understanding risk factor and pathophysiology to inform imaging and treatment. J Am Coll Cardiol 2016;68:2311-28.
Feng D, Glockner J, Kim K, et al. Cardiac magnetic resonance imaging pericardial late gadolinium enhancement and elevated inflammatory markers can predict the reversibility of constrictive pericarditis after anti-inflammatory medical therapy: a pilot study. Circulation 2011;124:1830-7.