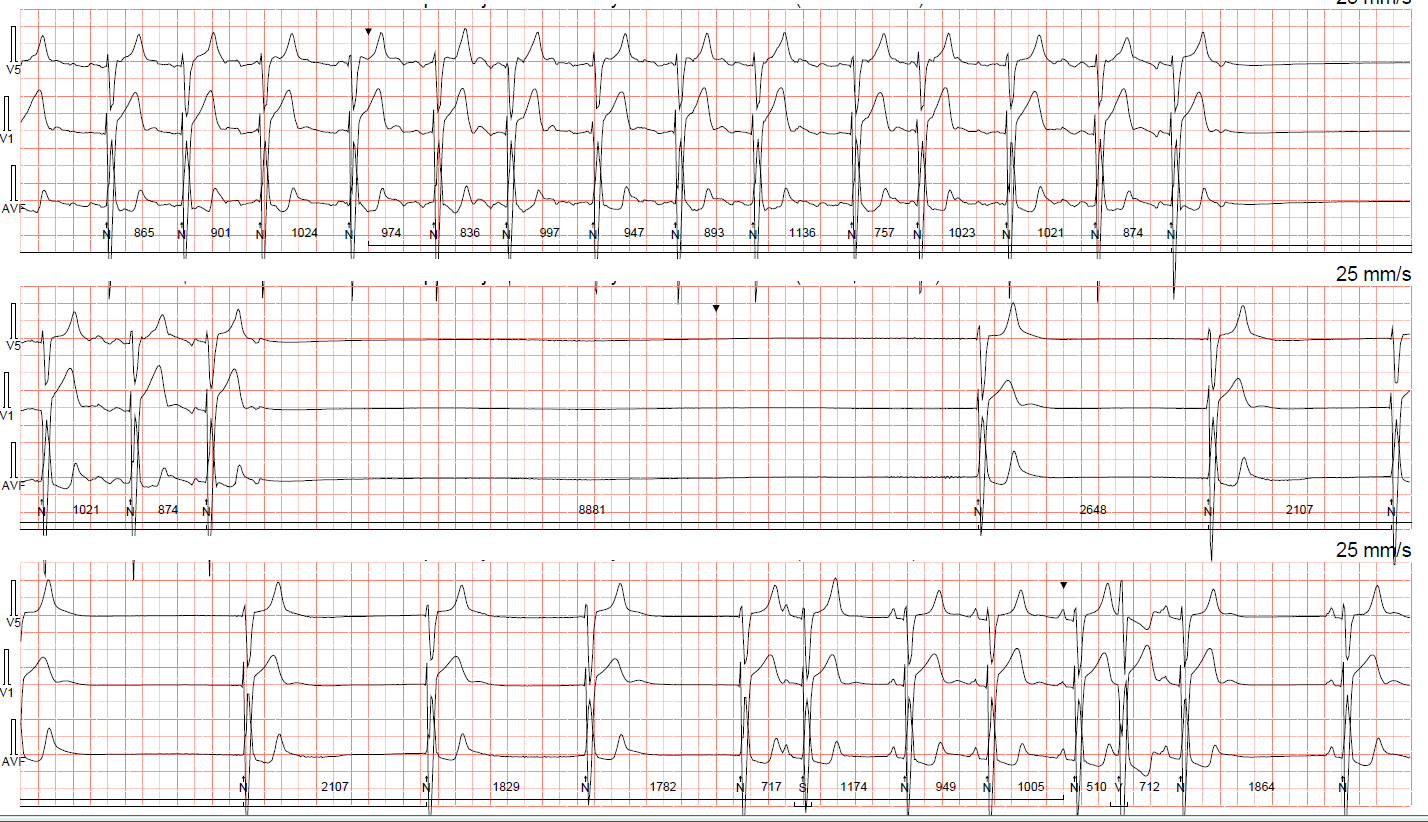
A 67-year-old female with a history of ischemic cardiomyopathy and paroxysmal atrial fibrillation presents with episodic palpitations and shortness of breath. Echocardiogram demonstrates stable left ventricular ejection fraction at 35-40% and severely enlarged left atrium. Current medications included metoprolol, digoxin, furosemide, simvastatin, rivaroxaban and aspirin. A Holter monitor is completed to evaluate her symptoms. The following tracing was recorded (Figure 1).
Figure 1
Which of the following is the most appropriate next step in her management?
Show Answer
The correct answer is: D. Permanent pacing is indicated.
The Holter monitor demonstrates atrial flutter that terminates spontaneously with sinus arrest followed by junctional escape. This is highly suggestive of sinus node dysfunction.
Sinus node dysfunction is associated with aging of the sinoatrial node and is predominantly related to fibrosis of the surrounding atrial tissue. It is frequently encountered in patients with atrial arrhythmias and has often been referred to as tachycardia-bradycardia syndrome in the literature. Short, et al. first described this syndrome in his seminal work published in 1954.1 The four patients in the original description had prolonged sinus pauses at the termination of atrial arrhythmias resulting in syncope.
Although the triggers and substrate for atrial fibrillation (AF) are predominantly in the left atrium, bi-atrial fibrosis is common and is thought to be one of the underlying mechanisms for sinus node dysfunction. Electrical remodeling due to brief paroxysms of AF has also been proposed as a potential mechanism.2 Permanent pacemaker implantation is the only option available for management of these patients. Current guidelines suggest it as a class I indication for symptomatic sinus node dysfunction or those who require continued use of negative chronotropic agents such as beta-blockers.3
Treatment of atrial fibrillation and flutter with catheter ablation or antiarrhythmic drugs to maintain sinus rhythm may be considered to help the symptoms associated with it; however, permanent pacing takes precedence as syncope due to sinus pauses may have catastrophic consequences. Similarly, rate control agents such as beta-blockers may further exacerbate sinus node dysfunction and should not be used for rate control in the absence of permanent pacing.
References
Short DS. The syndrome of alternating bradycardia and tachycardia. Br Heart J 1954;16:208-14.
John RM, Kumar S. Sinus Node and Atrial Arrhythmias. Circulation 2016;133:1892-900.
Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol 2008;51:e1-62.