An 18-year-old Caucasian female collegiate distance runner was referred to sports cardiology after an "abnormal family history" was obtained during her pre-participation screening exam. She had no significant past medical or surgical history and her only medication was oral contraceptive pills. She reported a family history of "sudden cardiac death" of her paternal grandfather at the age of 48, but was unclear of the actual details surrounding this event. On exam, she weighed 57kg, blood pressure was 103/66 mm Hg and her cardiovascular exam was normal.
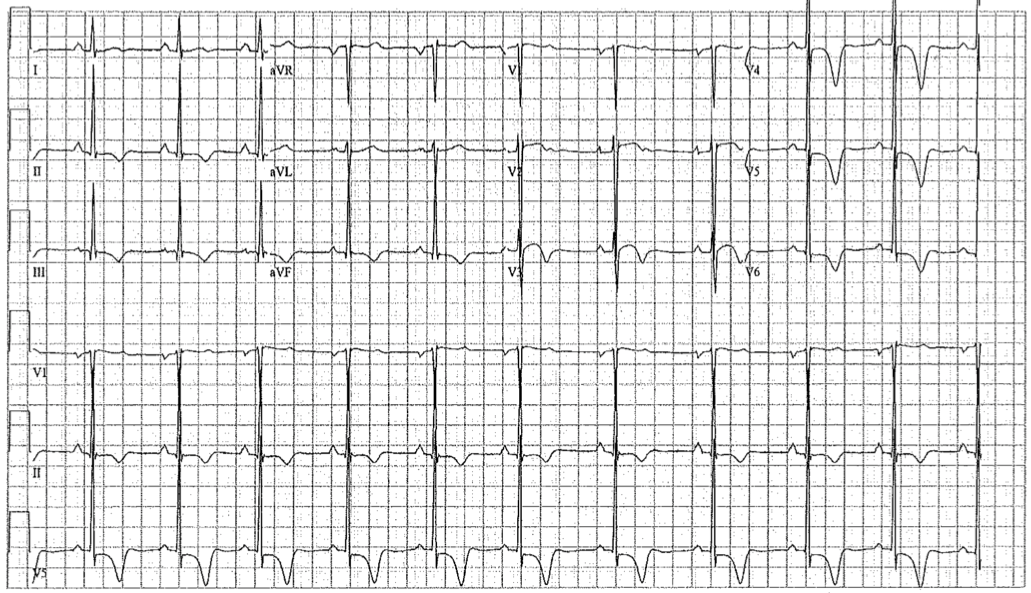
12-lead ECG:
Which of the following is an appropriate next step in her evaluation?
Show Answer
The correct answer is: D. In terms of imaging, cardiac MRI (CMR) is necessary as an adjunct to echocardiography.
This patient's resting electrocardiogram (ECG) demonstrates abnormal T-wave inversions (TWI) in the inferior limb leads and the anterolateral precordial leads. Given the possibility of underlying cardiomyopathy, inferior and/or lateral TWI are considered abnormal and further evaluation is necessary.1 Although TWI can be common findings on the screening ECG in athletic patients,2-5 this patient's ECG may be indicative of underlying structural cardiac pathology, particularly those cardiomyopathies that are genetically inherited. While trans-thoracic echocardiography (TTE) remains the mainstay imaging modality considered first line in the evaluation of athletes presenting with diffuse TWI, CMR is superior in detecting apical HCM, LVH localized to the lateral free wall, arrhythmogenic right ventricular cardiomyopathy with predominant LV involvement and myocarditis. As such, based on the International Recommendations for ECG Interpretation in Athletes,1 for athletes with inferolateral TWI, in addition to TTE, CMR is recommended as part of the routine diagnostic imaging algorithm. When CMR is not available, echocardiography with contrast should be considered as an alternative investigation for apical HCM in patients with deep TWI in leads V5-V6.
A second concern in this case is the possibility that these TWI represent a quiescent, or developing, cardiomyopathy. While there are multiple studies estimating the prevalence of TWI in young athletic cohorts, few have included long-term follow up of athletes with normal imaging studies. In one important study, out of 12,550 athletes with 123 demonstrating abnormal TWI, 39 athletes (32%) showed structural heart disease on initial imaging. Of the remaining 81 athletes with normal imaging, follow up evaluation (mean 9±7 years) demonstrated that five of these athletes (6%) progressed to a pathologic cardiovascular outcome.6 Similarly in a second large study by Schnell and colleagues, out of 6,372 athletes, 86 were identified as having pathologic TWI and normal imaging. During follow up evaluation, five athletes (7.2%) developed a cardiomyopathy.7 Based on these data, follow up evaluation and imaging on an annual basis throughout the athletic career is also recommended for athletes with inferolateral TWI and normal imaging.1
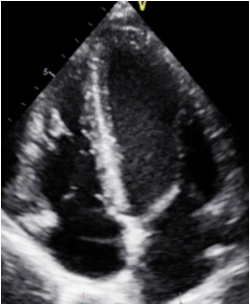
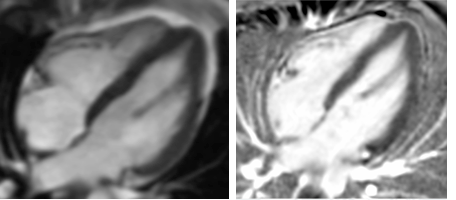
In this case, during the athlete's initial evaluation, a TTE showed normal biventricular size and function (Figure 1). CMR confirmed these findings and also excluded the presence of underlying myocardial fibrosis (Figure 2). The athlete was allowed to participate without restriction and completed the season with no cardiovascular complications. On her first annual follow-up, there were no changes noted on her ECG or imaging studies. She continues to participate in distance running without restriction and will follow up on an annual basis.
Sharma S, Drezner JA, Baggish A, et al. International recommendations for electrocardiographic interpretation in athletes. J Am Coll Cardiol 2017;69:1057-75.
Rawlins J, Carre F, Kervio G, et al. Ethnic differences in physiological cardiac adaptation to intense physical exercise in highly trained female athletes. Circulation 2010;121:1078-85.
Papadakis M, Basavarajaiah S, Rawlins J, et al. Prevalence and significance of T-wave inversions in predominantly Caucasian adolescent athletes. Eur Heart J 2009;30:1728-35.
Chandra N, Bastiaenen R, Papadakis M, et al. Prevalence of electrocardiographic anomalies in young individuals: relevance to a nationwide cardiac screening program. J Am Coll Cardiol 2014;63:2028-34.
Sheikh N, Papadakis M, Ghani S, et al. Comparison of electrocardiographic criteria for the detection of cardiac abnormalities in elite black and white athletes. Circulation 2014;129:1637-49.
Pelliccia A, Di Paolo FM, Quattrini FM, et al. Outcomes in athletes with marked ECG repolarization abnormalities. N Engl J Med 2008;358:152-61.
Schnell F, Riding N, O'Hanlon R, et al. Recognition and significance of pathological T-wave inversions in athletes. Circulation 2015;131:165-73.