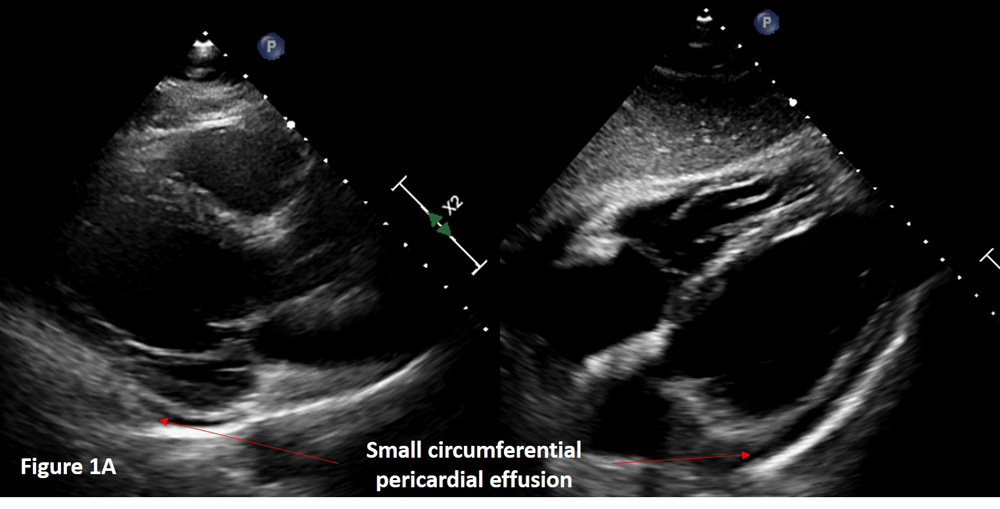
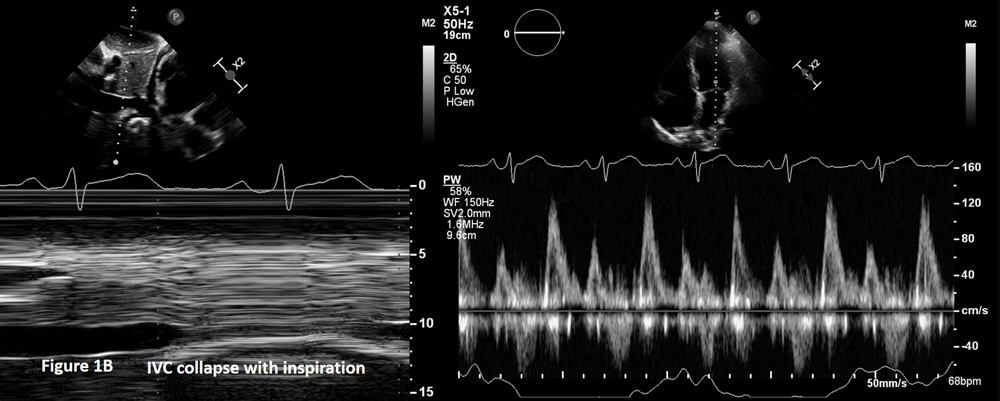
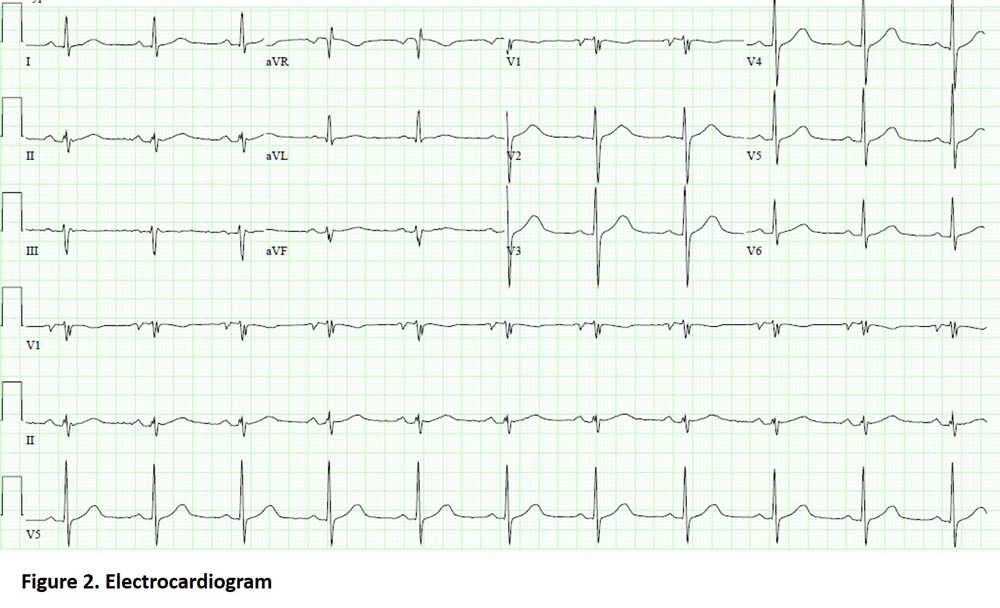
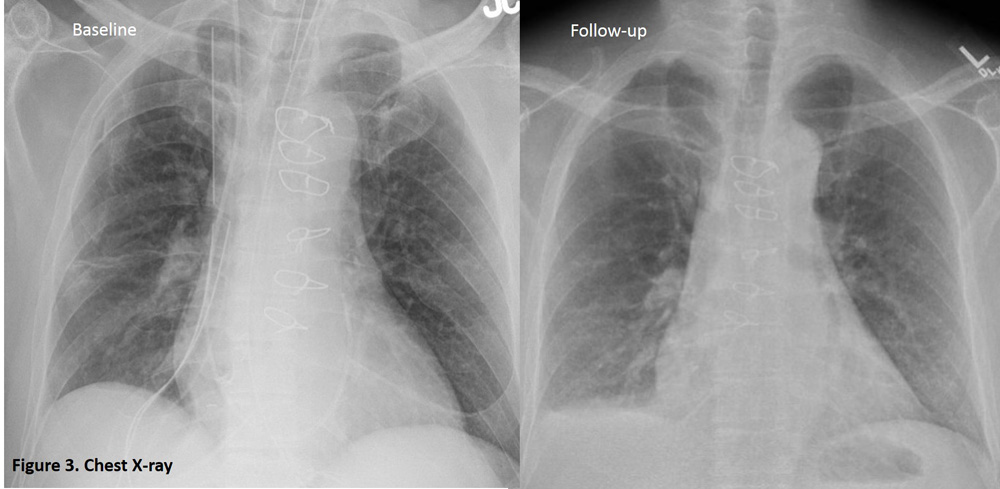
A 53-year-old man underwent sternotomy and subsequent replacement of the ascending aorta with aortic valve repair for ascending aortic aneurysm. He developed atrial fibrillation postoperatively and was started on amiodarone. A follow-up echocardiogram performed ten days later showed a small circumferential pericardial effusion with no echocardiographic evidence of tamponade (Figures 1A and 1B). He was asymptomatic with no fever, chest discomfort, shortness of breath or dizziness. Physical examination revealed normal vital signs (temperature 37.1°C, blood pressure 111/63 mmHg, heart rate 67 beats per minute, oxygen saturation of 97% on room air by pulse oximetry), normal jugular venous pressure, normal heart sounds, absence of pericardial friction rub, Kussmaul sign or lower extremity edema and a normal lung examination. Electrocardiogram and chest x-rays are shown (Figures 2 and 3). Erythrocyte sedimentation rate (ESR) was 97 mm/hour (reference range for normal, 0-15 mm/hour) and the C-reactive protein (CRP) was 4.5 mg/dL (reference range for normal, < 0.9 mg/dL).
Figure 1A
Figure 1B
Figure 2
Figure 3
Which of the following is true?
Show Answer
The correct answer is: C. Postpericardiotomy administration of colchicine has been shown to reduce the incidence of post-pericardiotomy syndrome but is not routinely recommended for prophylaxis.
The patient's electrocardiogram shows normal sinus rhythm and no evidence of pericarditis. Chest x-ray demonstrates presence of new small right sided pleural effusion. This patient meets criteria for postpericardiotomy syndrome based on presence of pericardial and pleural effusion and elevated CRP. According to the 2015 European Society of Cardiology guidelines for the diagnosis and management of pericardial diseases, the diagnosis of post-cardiac injury syndrome (PCIS) may be made after a cardiac injury if at least two of the following criteria are fulfilled: fever without alternative causes, pericarditic or pleuritic chest pain, pericardial or pleural rubs, evidence of pericardial effusion and/or pleural effusion, with elevated CRP.1 Post-cardiac injury syndrome is an umbrella terminology used to describe post-myocardial infarction pericarditis, postpericardiotomy syndrome (PPS) or post-traumatic pericarditis. PPS occurs after surgical trauma and inflammation being the hallmark of this condition. Data from two randomized control trials and a meta-analysis has established the efficacy of colchicine in the prevention of PPS when started in the post-operative or pre-operative period. The COPPS (COlchicine for Prevention of the Post-pericardiotomy Syndrome) multicenter trial randomized 360 patients to receive 1 mg colchicine loading dose or placebo on the third post-operative day with maintenance dose of 0.5 mg twice daily colchicine or placebo for 1 month (dosages were halved if body weight was less than 70 kilogram).2 The incidence of the primary efficacy endpoint, which was the occurrence of PPS at 12 months, was reduced in those who received colchicine as compared to placebo (8.9% vs. 21.1%; p= 0.002). Subsequently, the COPPS-2 (COlchicine for Prevention of the Post-pericardiotomy Syndrome and Post-operative Atrial Fibrillation) randomized controlled multicenter trial was performed to test the efficacy of colchicine for prevention of both PPS as well as post-operative atrial fibrillation. In this trial, colchicine at a dose of 0.5 mg twice daily (once daily for those with body weight less than 70 kilogram) was started 48 to 72 hours before surgery and continued for a month. The results showed significantly reduced incidence of PPS at 3 months, a primary efficacy endpoint of the study, when compared to placebo (19.4% vs. 29.4%; absolute difference, 10.0%; 95% confidence interval, 1.1%-18.7%), but no difference in the incidence of post-operative atrial fibrillation, a main secondary endpoint.3 However, the incidence of gastroenterological side effects was significantly higher as compared to placebo (14.4% vs. 6.7%; absolute difference, 7.7%; 95% confidence interval, 1.4%-14.3%) and therefore, colchicine is not routinely recommended for the prevention of PPS in patients undergoing surgery.
Based on the patient's initial presentation with new pericardial and pleural effusions and elevated levels of CRP and ESR, colchicine was considered but was not started in view of ongoing amiodarone therapy for post-operative atrial fibrillation. He received high-dose oral ibuprofen treatment but was subsequently hospitalized with chest pain and a large pericardial effusion that was successfully drained under echocardiographic guidance.
References
Adler Y, Charron P, Imazio M, et al. 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921-64.
Imazio M, Trinchero R, Brucato A, et al. COlchicine for the Prevention of the Post-pericardiotomy Syndrome (COPPS): a multicentre, randomized, double-blind, placebo-controlled trial. Eur Heart J 2010;31:2749-54.
Imazio M, Brucato A, Ferrazzi P, et al. Colchicine for prevention of postpericardiotomy syndrome and postoperative atrial fibrillation: the COPPS-2 randomized clinical trial. JAMA 2014;312:1016-23.