An 81-year-old man with stage IV lung adenocarcinoma presented with several weeks of progressive dyspnea on exertion and fatigue. He began treatment with the immune checkpoint inhibitor pembrolizumab 6 weeks prior, receiving 2 doses. Prior treatment with carboplatin and pemetrexed caused intolerable nausea after 1 cycle.
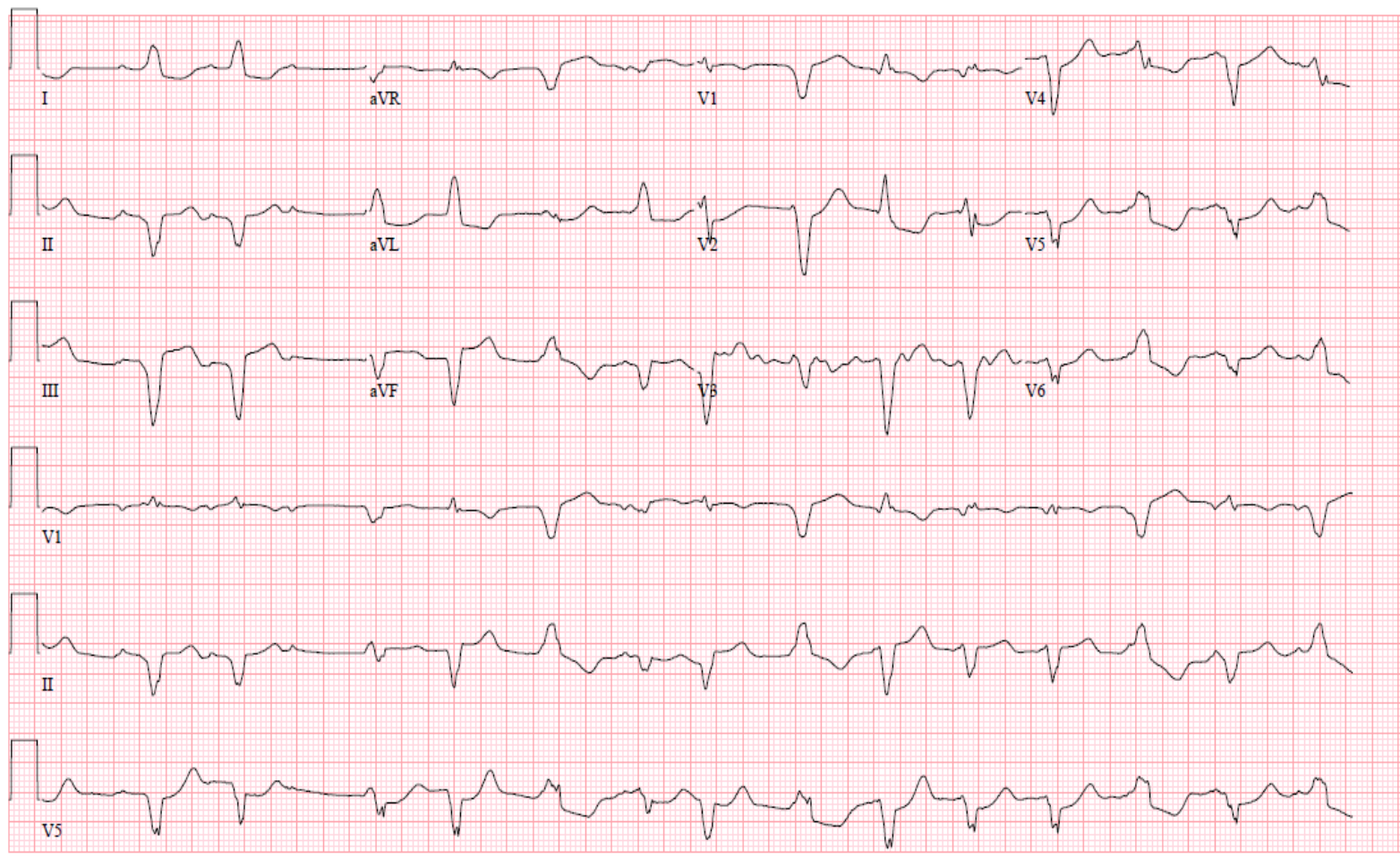
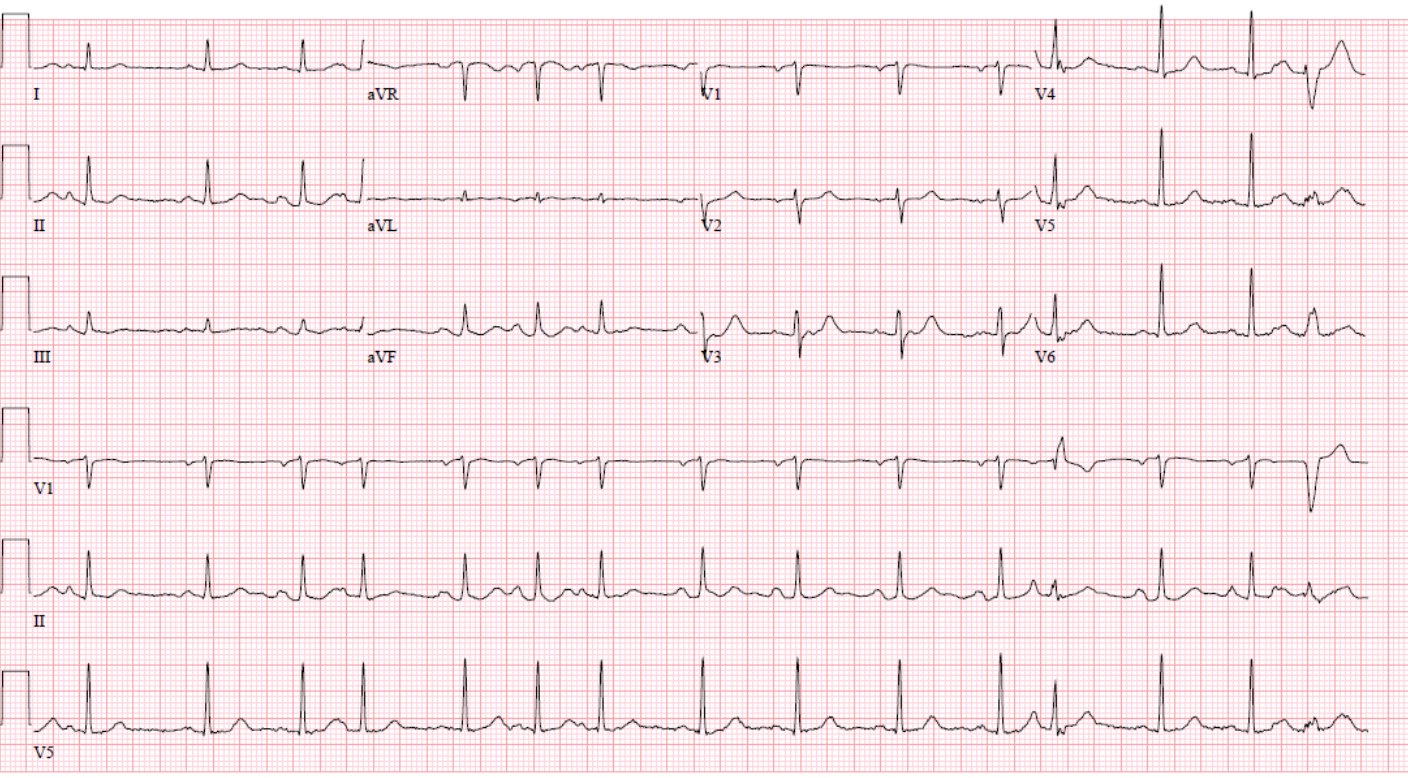
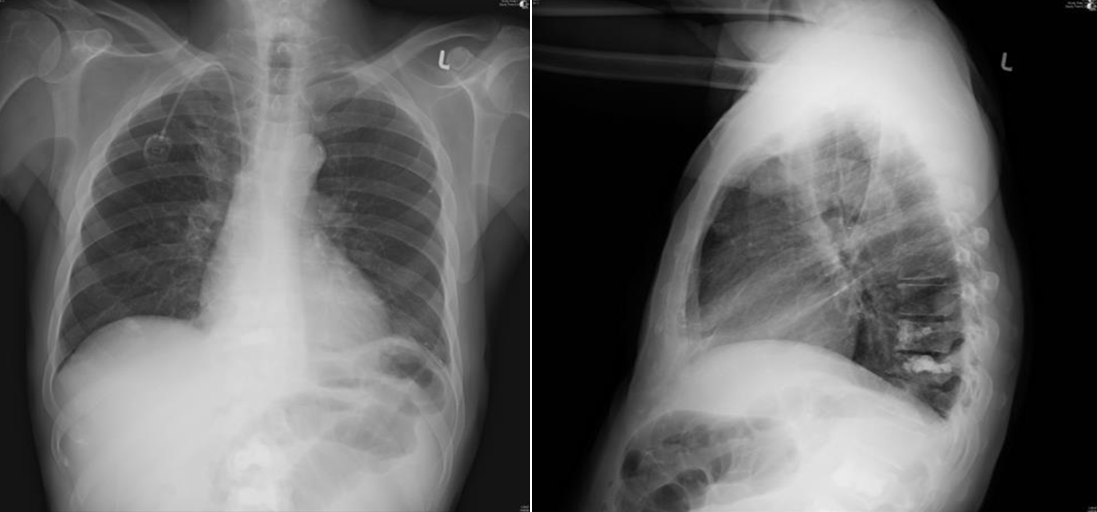
Initial examination was notable for normal vital signs and an irregular pulse. The chest was clear on auscultation, and there was no peripheral edema. The electrocardiogram (Figure 1) was significantly different from an earlier record (Figure 2). Chest radiograph showed clear lungs and no signs of heart failure or cardiac enlargement (Figure 3). Laboratory testing was notable for troponin-I 9.37 ng/mL (normal 0.00-0.50 ng/mL), creatine kinase-muscle/brain 102.7 ng/mL (normal 0.6-6.3 ng/mL), and brain natriuretic peptide 242 pg/mL (normal <101 pg/mL). C-reactive protein was 50 mg/L (normal <5 mg/L) and erythrocyte sedimentation rate 59 mm/hr. Cardiac catheterization with coronary angiography revealed no obstructive disease and decreased left ventricular (LV) function (ejection fraction [EF] ~40% and end-diastolic pressure 15 mmHg). He had a normal LVEF by echocardiography done 2 months earlier. Transthoracic echocardiography revealed new, diffuse biventricular dysfunction. Pulmonary ventilation/perfusion matching was low probability for pulmonary embolism.
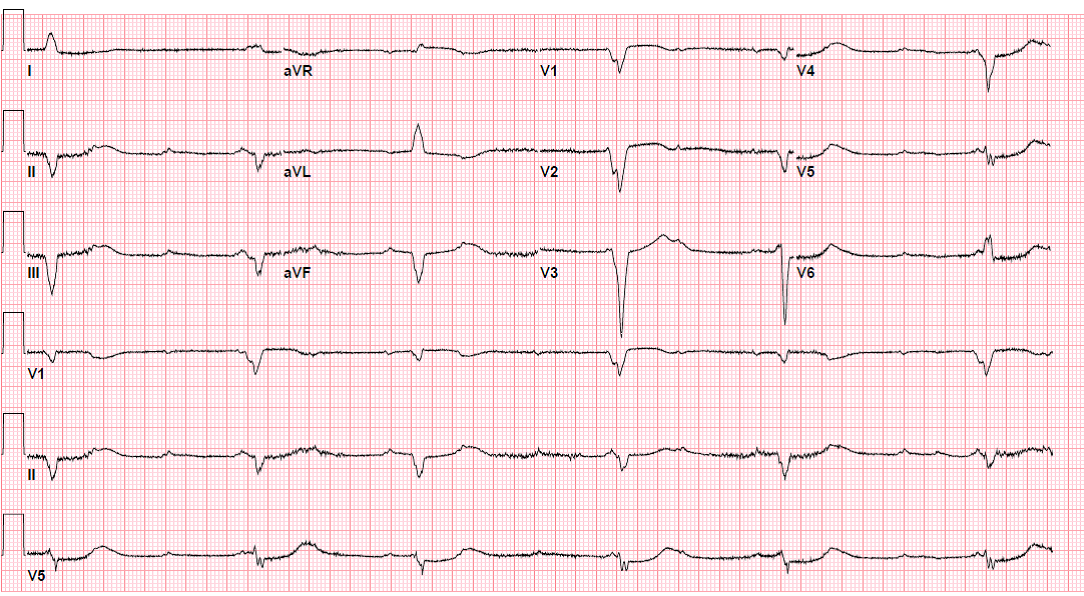
Overnight, he developed high-degree atrioventricular (AV) block requiring transvenous pacing (Figure 4). A permanent pacemaker was subsequently implanted after 4 days.
Figure 1
Figure 2
Figure 3
Figure 4
Which of the following is the most likely etiology of the patient's cardiomyopathy?
Show Answer
The correct answer is: D. Drug-induced myocarditis
Immune checkpoint inhibitors are a novel class of therapeutic agents associated with favorable responses in several cancers. Pembrolizumab, a programmed cell death receptor-1 blocking antibody, promotes antitumor immunologic responses by disrupting tumor cell inactivation of T-cells. Indications include treatment of patients with metastatic non-small cell lung cancer with adequate programmed death ligand-1 expression,1 and applications are expanding. Immune-related toxicities limit use and may affect any organ system.2 Myocarditis is relatively uncommon, reported in approximately 0.01% of patients in clinical trials, but the incidence may be underestimated.3 Histological analysis demonstrates intense, patchy lymphocytic infiltrates within the myocardium, often involving the AV nodes, and conduction system disease is a common feature.3
Immunohistochemical staining for the presence of diagnostic T-cell subtypes and absence of CD20 cells is helpful in excluding antibody-mediated inflammation. Pathology often exhibits predominantly macrophage infiltrates, distinct from other forms of myocarditis.4-6 Sub-fulminant or "smoldering" myocarditis following treatment initiation characterized by increased cardiac biomarkers or with electrical disturbance alone has also been described.7 Analysis of the biopsy sample by polymerase chain reaction can help exclude viral causes of myocarditis. Immune checkpoint inhibitor-associated cardiotoxicity tends to occur early; all cases reported to date have occurred within the first year of therapy, most after the first few infusions.3,5
For patients presenting with arrhythmias and conduction delay, early insertion of an intravenous pacemaker is important because the risk of progression to complete heart block is high. Corticosteroids are the mainstay of treatment, but prospective trials are lacking.8 Immunotherapy is stopped until symptoms resolve or indefinitely for high-grade toxicity.9 Clinical progression despite cessation of immunotherapy and treatment with corticosteroids is common, though limited data inform prognosis. Improvement in symptoms and ventricular function with corticosteroids has been reported,10 but survival remains limited by the underlying advanced malignancy.
Unfortunately, tissue biopsy was not obtained in this patient, who remained in heart block despite treatment with corticosteroids. Ventricular function improved to 48% by 4 weeks after initiation of high-dose corticosteroids, but he remained pacemaker-dependent months later. The implanted pacemaker was magnetic resonance imaging compatible, but the patient died in hospice before magnetic resonance imaging was performed.
Weber JS, Postow M, Lao CD, Schadendorf D. Management of Adverse Events Following Treatment With Anti-Programmed Death-1 Agents. Oncologist 2016;21:1230-40.
Johnson DB, Balko JM, Compton ML, et al. Fulminant Myocarditis with Combination Immune Checkpoint Blockade. N Engl J Med 2016;375:1749-55.
Wang DY, Okoye GD, Neilan TG, Johnson DB, Moslehi, JJ. Cardiovascular Toxicities Associated with Cancer Immunotherapies. Curr Cardiol Rep 2017;19:21.
Heinzerling L, Ott PA, Hodi FS, et al. Cardiotoxicity associated with CTLA4 and PD1 blocking immunotherapy. J Immunother Cancer 2016;4:50.
Norwood TG, Westbrook BC, Johnson DB, et al. Smoldering myocarditis following immune checkpoint blockade. J Immunother Cancer 2017;5:91.
Friedman CF, Proverbs-Singh TA, Postow MA. Treatment of the Immune-Related Adverse Effects of Immune Checkpoint Inhibitors: A Review. JAMA Oncol 2016;2:1346-53.
Puzanov I, Diab A, Abdallah K, et al. Managing toxicities associated with immune checkpoint inhibitors: consensus recommendations from the Society for Immunotherapy of Cancer (SITC) Toxicity Management Working Group. J Immunother Cancer 2017;5:95.
Läubli H, Balmelli C, Bossard M, Pfister O, Glatz K, Zippelius A. Acute heart failure due to autoimmune myocarditis under pembrolizumab treatment for metastatic melanoma. J Immunother Cancer 2015;3:11.