A 61-year-old woman with relapsed stage IV diffuse large B-cell lymphoma was admitted for haploidentical stem cell transplant (SCT). She had no known comorbidities or cardiac risk factors, and baseline electrocardiogram (ECG) and transthoracic echocardiogram (TTE) were normal. Her conditioning regimen comprised fludarabine, melphalan, and thiotepa. High-dose post-transplantation (PT) cyclophosphamide (CY) at 50 mg/kg/day (total 2500 mg/day) was given on days +3 and +4 for prevention of graft-versus-host disease (GVHD). After the first dose of PT-CY (day +3), she developed shortness of breath and hypoxia, requiring bi-level positive airway pressure support, and oliguric acute kidney injury, requiring continuous venovenous hemodialysis. After the second dose of PT-CY (day +4), she was placed on mechanical ventilation for worsening hypoxia and vasopressor support for hypotension. Physical exam revealed sinus tachycardia, a new holosystolic murmur, S3 gallop, bibasal rales, elevated jugular venous pressure to 10 cmH2O, and bilateral lower extremity pitting edema. Laboratory results were notable for severe pancytopenia, markedly high brain natriuretic peptide at 2450 pg/mL, and elevated cardiac troponin I with a peak of 0.68 ng/mL. ECG changes included diffuse T-wave inversions and low-voltage complexes (Figure 1), and TTE showed biventricular systolic dysfunction and global left ventricular (LV) hypokinesis with an ejection fraction of 16% (Figure 2). On day +5, her condition worsened despite vasopressors and inotropes, and the patient subsequently died.
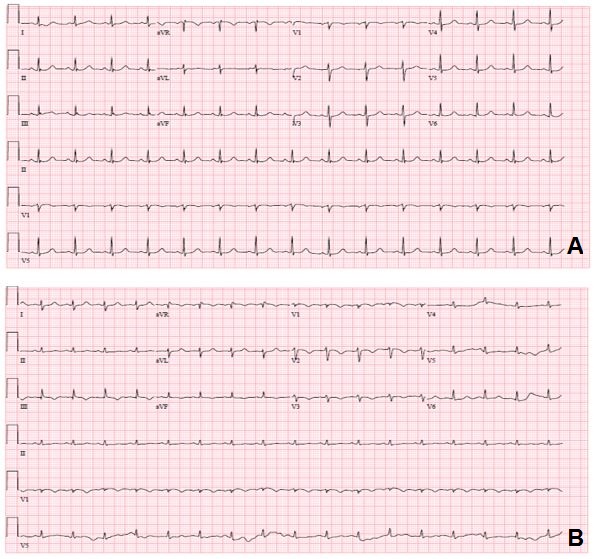
Figure 1
Comparison of (A) pre-treatment and (B) post-treatment ECGs.
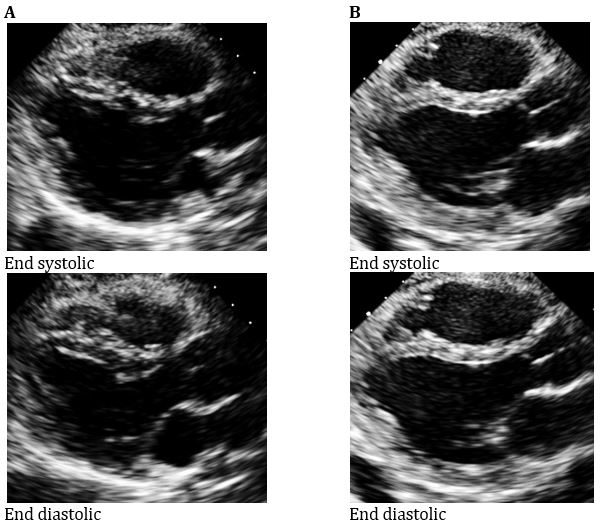
Figure 2
Comparison of (A) pre-treatment and (B) post-treatment echocardiograms.
What is the most common manifestation of CY cardiotoxicity?
Show Answer
The correct answer is: D. Hemorrhagic myopericarditis
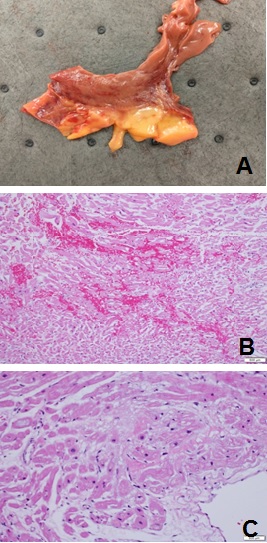
Although the incidence is rare, CY-induced cardiomyopathy presents with a histopathologic correlate characterized by hemorrhagic myopericarditis. Autopsy demonstrated cardiomegaly with LV hypertrophy and right ventricular enlargement. Coronary vessels were patent. Histopathologic exam revealed multifocal myocardial hemorrhages, myocyte vacuolization, contraction bands, and nuclear pyknosis, characteristic of acute myocardial injury from CY (Figure 3).
Figure 3: Cardiac Autopsy Macroscopic and Microscopic Examinations
Acute congestive heart failure (HF) is among the early cardiac events complicating SCT. It is typically associated with high-dose CY but has also been seen with the reduced intensity conditioning regimen of melphalan and fludarabine.1 CY is a DNA alkylating agent with antineoplastic and immunosuppressive properties.2,3 In the field of SCT, it is used as part of pre-transplant conditioning regimens and as post-transplant GVHD prophylaxis especially in haploidentical SCT cases, where it is dosed as 50 mg/kg/day for 2 days.4,5 Cardiomyopathy occurs as a consequence of high-dose CY. However, CY regimens vary according to disease, and the threshold for cardiotoxicity remains unclear. A review by Wadia proposed high dose to be ≥40 mg/kg/day or ≥1.4 mg/kg/day for at least 2 days.3
Hemorrhagic myocarditis (or myopericarditis) is a rare but fatal complication of high-dose CY that manifests as fulminant HF. CY is metabolized into both therapeutic and cytotoxic metabolites, and the latter are thought to cause endothelial and myocyte injury through oxidative damage. Symptoms usually develop within 2-10 days of drug administration. Typical findings include new low-voltage complexes on ECG, elevated cardiac biomarkers, and increased myocardial thickness, global LV or biventricular failure, and pericardial effusion on TTE. Characteristic histopathologic changes show capillary microthrombosis, interstitial hemorrhage and fibrin deposition, and myocyte necrosis.2-4,6,7 However, antemortem myocardial biopsy is precluded in most cases due to concurrent thrombocytopenia and other organ dysfunction. Other noninvasive methods such as cardiac magnetic resonance imaging have not yet been used to specifically characterize this type of myocarditis.2 At this time, treatment remains largely supportive to prevent refractory cardiogenic shock,2,3,6 although recent laboratory studies on N-acetylcysteine have shown positive cardioprotective effects against CY.4
A retrospective study by Lin et al. on 176 patients who underwent SCT with PT-CY showed a 21.9% incidence of PT cardiomyopathy, not significantly different from matched non-PT-CY patients. However, cause of death could not be ascertained among those who died.5 To our knowledge, this is the first histologically documented case of CY-induced hemorrhagic myocarditis in the setting of high-dose PT-CY. Given the non-specific nature of clinical and noninvasive diagnostic findings of myocarditis, this entity should be in the differential diagnosis of acute severe HF after high-dose CY administration due to its grave prognosis. A high clinical suspicion is key for timely initiation of therapy, including mechanical circulatory support modalities.
References
Blaes A, Konety S, Hurley P. Cardiovascular Complications of Hematopoietic Stem Cell Transplantation. Curr Treat Options Cardiovasc Med 2016;18:25.
Dhesi S, Chu MP, Blevins G, et al. Cyclophosphamide-Induced Cardiomyopathy: A Case Report, Review, and Recommendations for Management. J Investig Med High Impact Case Rep 2013;1:2324709613480346.
Wadia S. Acute Cyclophosphamide Hemorrhagic Myopericarditis: Dilemma Case Report, Literature Review and Proposed Diagnostic Criteria. J Clin Diagn Res 2015;9:OE01-OE3.
Kurauchi K, Nishikawa T, Miyahara E, Okamoto Y, Kawano Y. Role of metabolites of cyclophosphamide in cardiotoxicity. BMC Res Notes 2017;10:406.
Lin CJ, Vader JM, Slade M, DiPersio JF, Westervelt P, Romee R. Cardiomyopathy in patients after posttransplant cyclophosphamide-based hematopoietic cell transplantation. Cancer 2017;123:1800-9.
Ishida S, Doki N, Shingai N, et al. The clinical features of fatal cyclophosphamide-induced cardiotoxicity in a conditioning regimen for allogeneic hematopoietic stem cell transplantation (allo-HSCT). Ann Hematol 2016;95:1145-50.
Martin M, Fornecker LM, Marcellin L, et al. Acute and fatal cardiotoxicity following high-dose cyclophosphamide in a patient undergoing autologous stem cell transplantation for systemic sclerosis despite satisfactory cardiopulmonary screening. Bone Marrow Transplant 2017;52:1674-7.