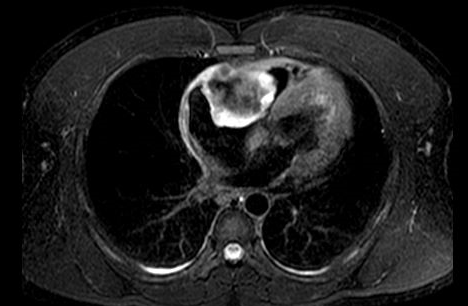
A 41-year-old man with no past medical history presented to the emergency department with 3 weeks of progressive headache. Additionally, he noted fatigue, dizziness, exertional dyspnea, and a 20-pound weight loss over the prior 6 months. Initial blood pressure was 206/140, and a heart murmur was heard over the left sternal border. A urine drug screen was positive for cocaine. A transthoracic echocardiogram showed a large right atrial mass, and subsequent transesophageal echocardiogram showed a heterogeneous mass measuring 5.6 x 4.6 cm that appeared to be attached to the right atrial appendage, lateral tricuspid valve annulus, and possibly right ventricle. The tricuspid valve was obscured by the mass, but an increased pressure gradient was noted with severe functional stenosis. Cardiac magnetic resonance imaging (CMRI) was concerning for angiosarcoma versus lymphoma (Figure 1).
Figure 1
Which of the following is true regarding the diagnosis and management of suspected cardiac tumors?
Show Answer
The correct answer is: A. The specific symptoms of cardiac tumors are generally determined by the tumor's size and location rather than its histopathology.
Primary cardiac tumors are extremely rare, with metastasis to the heart from other primary cancers being 30 times more common.1 Primary cardiac tumors can present with symptoms or be discovered incidentally during evaluation for other medical issues or routine physical exam. When symptoms exist, they are typically determined by the tumor's size and location rather than its histopathology. Presenting symptoms of cardiac tumors include congestive heart failure from intracardiac obstruction, systemic embolization, constitutional symptoms, and arrhythmias.
The diagnosis of cardiac tumors involves imaging, typically with echocardiograms and cardiac computed tomography (CT) or CMRI. A transthoracic echocardiogram is the simplest test for diagnosis, however CT and CMRI provide additional details. CMRI is generally recommended to assess extent of myocardial infiltration and to differentiate between benign (thrombus and myxoma) and malignant masses. Biopsy should be attempted on all malignant masses because some malignancies are best treated with chemotherapy alone, such as lymphoma, rather than surgical intervention.
About 75% of primary cardiac tumors are benign, and of the 25% that are malignant, approximately 75% are sarcomas.2 The majority of benign tumors are thrombus and myxomas, commonly arising in the left atrium. Myxomas should be managed with surgical resection due to the risk of tumor embolization and other complications. Malignant primary cardiac sarcomas are found in both sides of the heart, with the right atrium having more angiosarcoma and the left sided chambers with pleomorphic and leiomyosarcomas. Although the studies on treatment of malignant cardiac tumors is limited due to the rarity of the disease, the current consensus is that these tumors should be treated with a combination of surgical resection and neoadjuvant systemic chemotherapy prior to resection. Total resection can be difficult depending on the extent of the tumor's involvement with cardiac structures. Survival is based on ability to achieve negative surgical margins and can extend mean life expectancy to 3-5 years at least. Without surgical resection, primary cardiac tumors have a very poor prognosis, with a survival rate of only 10% at 9-12 months. Cardiac tumors should be managed at surgical centers with experience treating cardiac tumors because combined treatment with systemic chemotherapy and surgery can prolong survival. New techniques such as autotransplantation for cardiac tumors are emerging as are new chemotherapy options.3
In the above case, following the CMRI the patient underwent CT of chest, abdomen, and pelvis, which showed no evidence of metastatic disease. He was transferred to a tertiary care facility, and he underwent debulking surgery secondary to hemodynamic tricuspid valve stenosis. Pathology demonstrated extraskeletal fibroblastic osteosarcoma, a very rare diagnosis. Follow-up CMRI demonstrated a decrease in size of the atrial mass following debulking to 4.9 x 3.2 cm; however, there was resultant severe tricuspid regurgitation due to marked failure of coaptation. He was referred to oncology and started chemotherapy consisting of adriamycin and olaratumab. His treatment course was complicated by an interval increase in size of the atrial tumor consistent with progression of disease, necessitating alternative chemotherapy.
References
Leja MJ, Shah DJ, Reardon MJ. Primary cardiac tumors. Tex Heart Inst J 2011;38:261-2.
Yusuf SW, Reardon MJ, Banchs J. Cardiac tumors. Cardiology 2014;129:197–8.
Abu Saleh WK, Ramlawi B, Shapira OM, et al. Improved Outcomes With the Evolution of a Neoadjuvant Chemotherapy Approach to Right Heart Sarcoma. Ann Thorac Surg 2017;104:90-7.