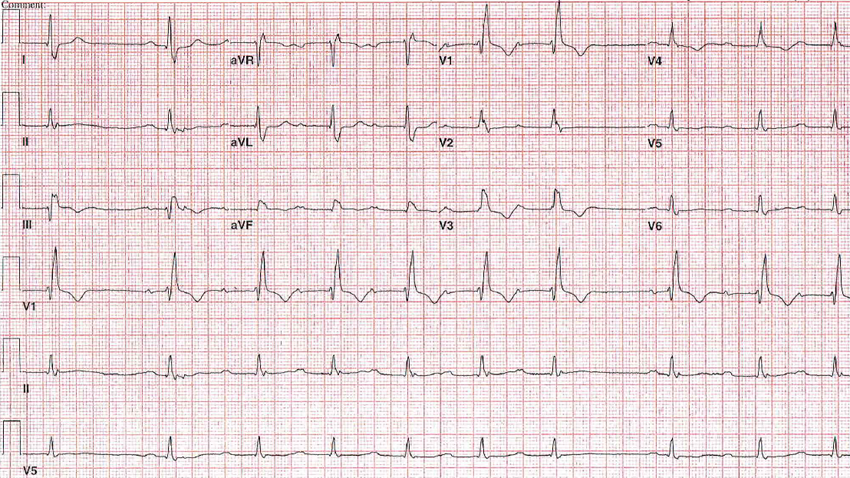
An 84-year-old man presents with a history of hypertension, hyperlipidemia, and bladder cancer. He is undergoing outpatient chemotherapy. He is seen due to persistent anterior chest discomfort and shortness of breath. An echocardiogram shows mild aortic stenosis with normal left ventricular function. Coronary angiography is performed; aan LAD in-stent stenosis of 80% is dilated and stented. A post procedure electrocardiogram (ECG) (Figure 1) is performed.
Figure 1
Figure 1
The ECG shows right bundle branch block (RBBB) and which of the following?
Show Answer
The correct answer is: C. Dual AV node physiology/pause.
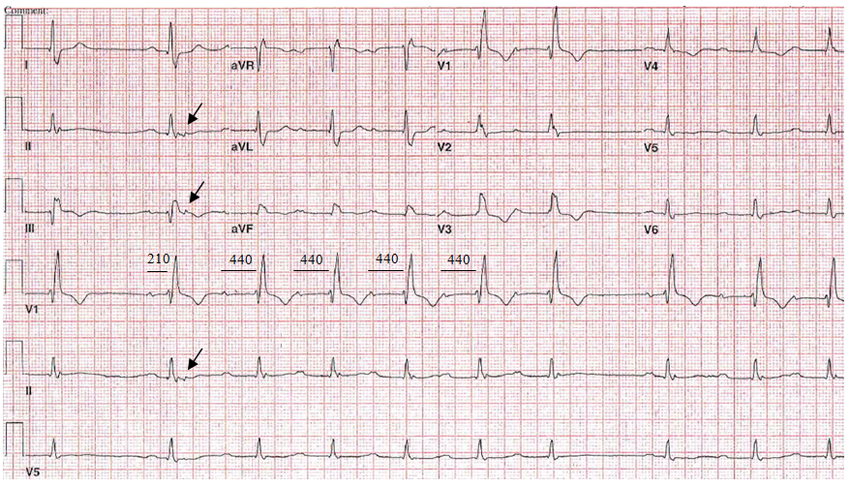
There is sinus rhythm/sinus bradycardia with two PR intervals: one relatively short (210 ms) and the other relatively long (440 ms). These represent dual AV node physiology (fast and slow pathways). There is an ectopic P wave just after the second QRS, which could be blocked PAC (arrow) in the fast pathway or blocked His-extrasystole. This premature beat seems to set off the run of long PRs with conduction down the slow pathway. Then, conduction blocks in the slow pathway, and pause and conduction resumes for one beat over the fast pathway. See Figure 2. This could be confirmed in the EP lab; however, this was not done in this case.
Answer A is incorrect due to the absence of progressive prolongation of PR and the absence of blocked P wave at the end of group beats.
Figure 2
Figure 2
Additionally, RBBB is present. Inferior infarction is not present, and a significant Q wave is also not present in aVF.
There is probably left atrial abnormality (LAA) and may be some slight wandering atrial pacemaker.
References
Viljoen C, Smith R, Chin A. Reviewing the causes of electrocardiographic pauses. Cardiovasc J Afr 2017;28:257-60.
Wung SF. Bradyarrhythmias: Clinical Presentation, Diagnosis, and Management. Crit Care Nurs Clin North Am 2016;28:297-308.