A 72-year-old male Chinese Han patient presented to emergency department with sudden chest pain for 2 hours. He has a longstanding history of hypertension, diabetes, hyperlipidemia, cigarette smoking, and polycythemia vera (PV) with JAK2 V617F mutation for 7 years. Hydroxyurea was prescribed as a cytoreductive therapy. On review of his medical history, he had experienced 3 cardiac events in the past 12 years (Tables 1-2).
Table 1: Laboratory Findings in Previous Cardiac Events
Laboratory examination
Apr 2005
Dec 2005
Sep 2010
White blood cell (× 109/L)
9.47
13.65
16.48
Hemoglobin (g/L)
167
178
185
Hematocrit (%)
51
53
58.3
Thrombocytes (× 109/L)
547
448
559
High sensitive C reactive protein (mg/L)
4.87
3.02
-
Low-density lipoprotein (mg/dL)
112
63
91
High-density lipoprotein (mg/dL)
38
38
29
Table 2: Coronary Angiographic Findings, Intervention, and Outcomes in the Previous Cardiac Events
Accessory Examination
Apr 2005
Dec 2005
Sep 2010
Coronary angiography findings
Left main coronary artery (LM) (-)
Left anterior descending branch artery (LAD) proximal 40% stenosis
Left circumflex branch artery (LCX) (-)
Right coronary artery (RCA) (-)
Aspirin alone following combination with clopidogrel 3 months later
Aspirin, clopidogrel
Outcomes
No complications
No complications
Bleeding Academic Research Consortium Type 2 bleeding
(gingival bleeding and cutaneous hematoma)
6 months later
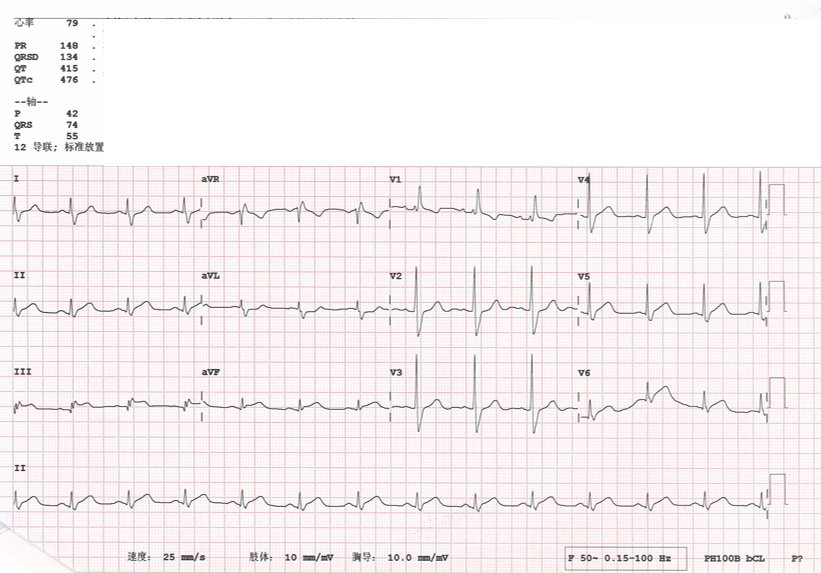
In addition to mild facial hyperemia and hepatosplenomegaly, no obvious abnormalities were found in the physical examination. Electrocardiography (ECG) on admission revealed a marked ST-segment elevation in leads Ⅱ, Ⅲ, aVF, and V5-V6 (Figure 1). The preliminary diagnosis was acute ST-segment elevation myocardial infarction (STEMI) involving the left ventricular inferior and lateral walls. Complete blood count analysis was as follows:
White blood cell count = 19.41 × 109/L
Hemoglobin = 143g/L
Red blood cell count = 4.97 × 1012/L
Hematocrit = 41.8%
Thrombocytes = 530 × 1012/L
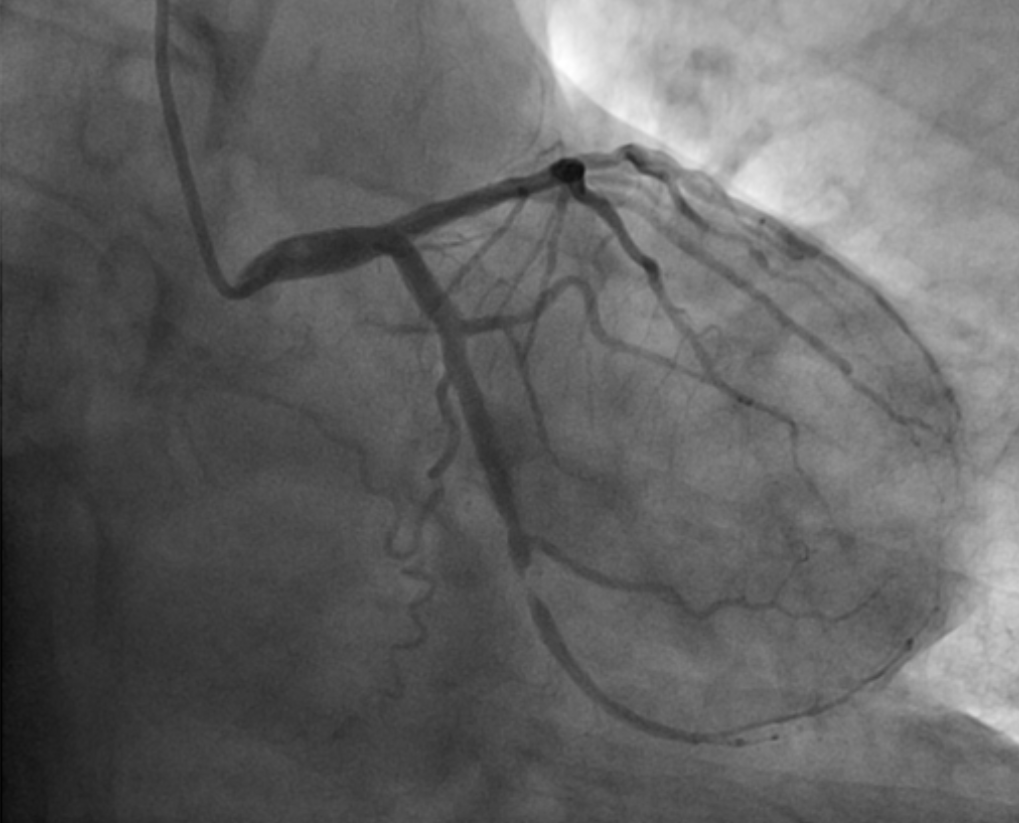
The level of cardiac-specific troponin I was 0.077 mcg/L (normal range: 0-0.056 mcg/L). Other initial laboratory tests revealed normal clotting screen, electrolytes, serum urea, and creatinine. A loading dose of aspirin and clopidogrel (300 mg each) was given immediately. Emergency coronary angiogram results are shown in Figure 2.
Figure 1: ECG on Admission (2 Hours After Chest Pain)
Figure 1
Figure 2: Emergency Coronary Angiogram Results
Figure 2
Based on the clinical presentation, laboratory tests, and coronary catheterization, what is the most likely mechanism for this patient's STEMI?
Show Answer
The correct answer is: A. Late stent thrombosis
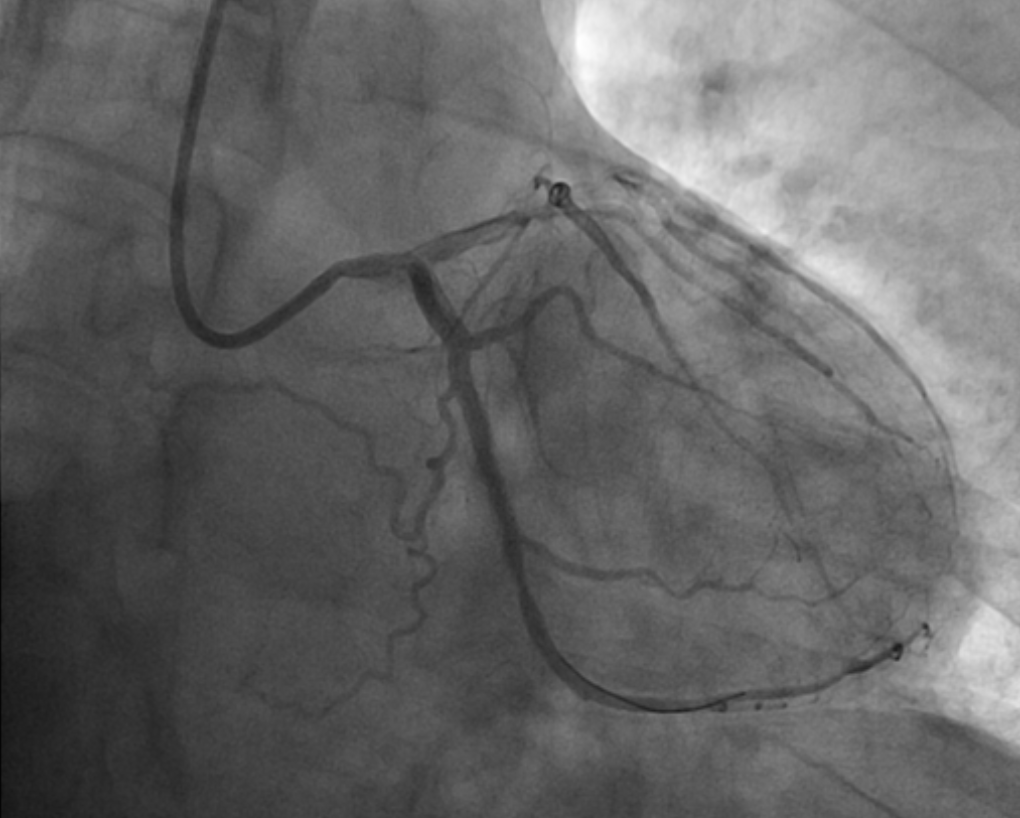
Because the culprit lesion was localized to the mid-LCX, he was treated with balloon angioplasty. We considered the cause of myocardial infarction to be very late stent thrombosis because the patient underwent stent implantation 7 years prior, and the culprit lesion was at the distal end of original stent. The LCX was successfully recanalized by balloon dilation but without any stent implantation. The final angiogram showed 20% residual stenosis with Thrombolysis In Myocardial Infarction 3 flow (Figure 3). ECG later indicated that resolution of the ST-segment elevation. The level of troponin I peaked at 34.85 mcg/L, 7 hours after the onset of chest pain. The patient was given oral treatment with aspirin 100 mg/d, clopidogrel 75 mg/d, and subcutaneous injection of enoxaparin 6000 U every 12 hours for 3 days. The patient recovered well over the next 60 days.
Figure 3: Post-Balloon Dilation Angiographic Result
Figure 3
PV, characterized by erythrocytosis and thrombocytosis, is listed by the World Health Organization as Philadelphia chromosome-negative chronic myeloproliferative neoplasm. Other features include leukocytosis, splenomegaly, thrombosis, bleeding, microcirculatory symptoms, pruritus, and risk of leukemic or fibrotic transformation. Clinical characteristics affecting overall survival in PV include advanced age, leukocytosis, and thrombosis. Age >60 years and thrombosis history are the two main risk factors for recurrent vascular events. Currently, the main goal of therapy in PV is to prevent thrombotic complications without increasing bleeding risk.1 Acute coronary syndrome (ACS) is an example of an arterial thrombosis event and a severe complication of PV that should be treated immediately. Because of the rarity of the disease and lack of large cohort studies data, the literature describing PV complicated by ACS is limited to case reports.
In addition, very late stent thrombosis has also been reported in patients with coronary heart disease alone. The leading mechanism of very late stent thrombosis was attributed to malapposed struts, rupture of neoatherosclerotic neointima, and discontinuation of antiplatelet agents.2,3 It is notable that the patient had discontinued antiplatelet agents due to the complication of previous minor bleeding.
To our knowledge, optimal pharmacologic and interventional management strategies remain unclear. Several cases reported on PubMed in the past 5 years are listed in Table 3.4-9 Of these 6 patients, 5 experienced STEMI and 1 experienced unstable angina pectoris. Stent implantation was performed in 2 patients, and stent thrombosis occurred in both patients after the intervention, one several hours later and the other 3 days later. Acute bridge thrombosis formed in 1 of the other 2 patients who underwent coronary artery bypass grafting (CABG). The remaining 2 cases had better outcomes, of which 1 underwent thrombolysis with reteplase and the other was treated with simple drug treatment.
Table 3: Cases Reported on PubMed in the Past 5 Years
Elective single CABG, ongoing antiplatelet therapy
None
Osada9
M
65
Unstable angina pectoris
CABG
Aspirin, heparin
Thrombotic stenosis and remedial stent implantation
Through our retrospective analysis of the literature and based on our own clinical practice, we propose that in the era of interventional therapy as a mainstream strategy, stent implantation may not be the optimal choice for patients with PV and ACS. Once the stent is implanted, the intracoronary and systemic thrombotic environment could lead to an increased risk of stent thrombosis. Also, the inevitable enhanced antiplatelet therapy may increase the risk of bleeding.
Regarding antithrombotic therapy, treatment should be tailored to the individual patient to balance the risk of thrombosis and bleeding. For patients with PV, low-dose aspirin (81 mg/day; range 40-100 mg/day) is the standard drug treatment and is recommended by the guidelines.1 A recent case-control study suggests that direct oral anticoagulants may be highly effective and safe for use in patients with Philadelphia chromosome-negative chronic myeloproliferative neoplasm. For ACS, anticoagulation is clearly recommended in the guidelines.10 However, there are no guidelines available for treatment of PV complicated by ACS. The antithrombotic strategy may differ based on the patient's clinical condition and reperfusion method. The risk of thrombosis and bleeding should be carefully weighed to determine the individualized antithrombotic strategy.
References
Tefferi A, Barbui T. Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management. Am J Hematol 2017;92:94-108.
Souteyrand G, Amabile N, Mangin L, et al. Mechanisms of stent thrombosis analysed by optical coherence tomography: insights from the national PESTO French registry. Eur Heart J 2016;37:1208-16.
McFadden EP, Stabile E, Regar E, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004;364:1519-21.
Gouri A, Yakhlef A, Dekaken A, Bentorki AA. Acute myocardial infarction revealing a polycythemia vera. Ann Biol Clin (Paris) 2012;70:489-91.
Bahbahani H, Aljenaee K, Bella A. Polycythemia vera presenting as acute myocardial infarction: An unusual presentation. J Saudi Heart Assoc 2015;27:57-60.
Inami T, Okabe M, Matsushita M, et al. JAK2 mutation and acute coronary syndrome complicated with stent thrombosis. Heart Vessels 2016;31:1714-6.
Zhang W, Zhang Y, Liu Y, et al. Acute ST-elevation myocardial infarction in a patient with polycythemia vera. Chin Med J (Engl) 2014;127:397.
Nahler A, Fuchs D, Reiter C, Kiblböck D, Steinwender C, Lambert T. Myocardial infarction with proximal occlusion of the left anterior descending coronary artery in a 22-year-old patient with polycythaemia vera. Clin Med (Lond) 2017;17:46-7.
Osada H, Nakajima H, Meshii K, Ohnaka M. Acute coronary artery bypass graft failure in a patient with polycythemia vera. Asian Cardiovasc Thorac Ann 2016;24:175-7.
Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients With Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2016;68:1082-155.