A 39-year-old Caucasian female was referred to cardiology clinic for evaluation of new onset hypertension. She had no significant past medical history but had two ER visits within the preceding month for hypertensive urgency prompting initiation of three anti-hypertensive medications: carvedilol 25mg BID, amlodipine 10mg daily and hydrochlorothiazide 25mg daily. She reported symptoms of intermittent headaches and pulsatile tinnitus. She had no family history of hypertension. On physical exam, blood pressure was 202/112 mmHg, and the remainder of her exam was normal. Initial laboratory evaluation showed normal creatinine, erythrocyte sedimentation rate (ESR) and C-reactive protein. Further laboratory testing for hyperthyroidism, hyperaldosteronism and pheochromocytoma were all negative. Renal artery duplex ultrasound showed normal sized kidneys, but there were elevated Doppler velocities in the left renal artery concerning for left renal artery stenosis. Thus, the patient was referred for renal angiogram. The notable findings are seen in Figure 1.
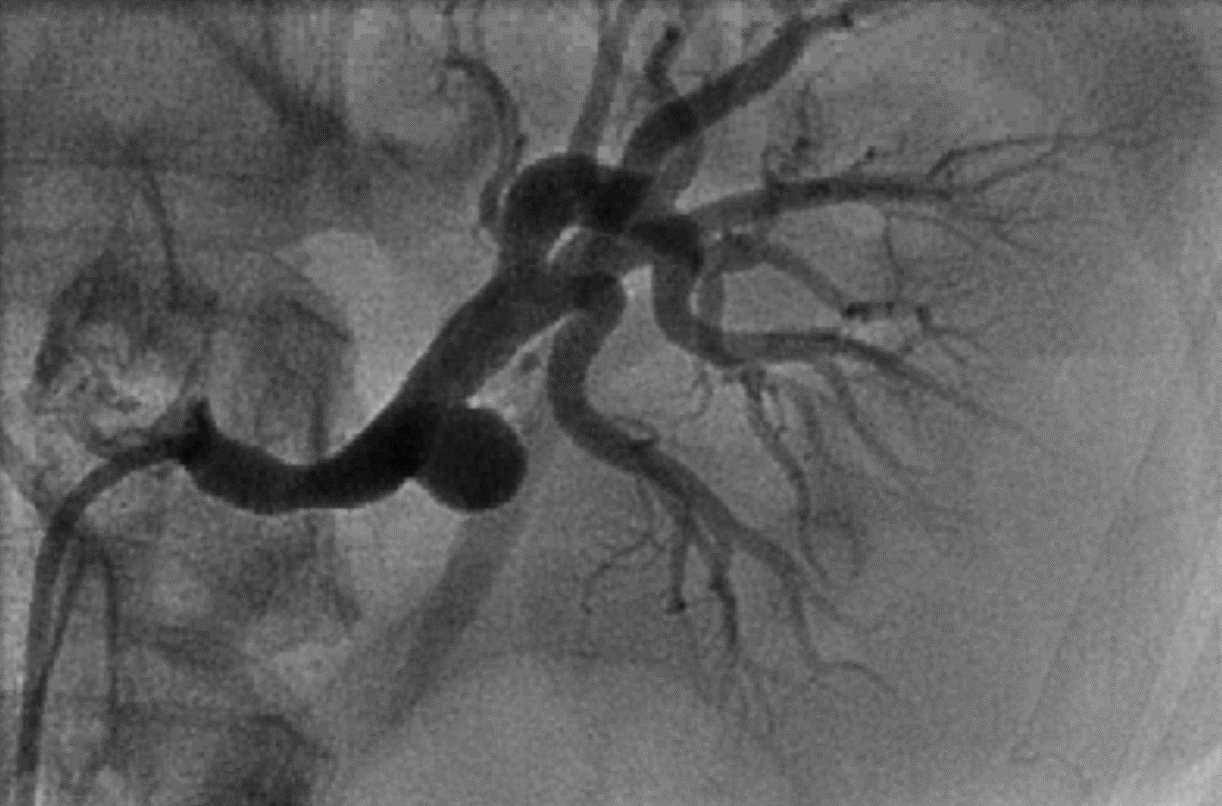
Figure 1: Renal Angiogram
Figure 1
Which of the following is the most likely etiology for this patient's left renal artery abnormalities?
Show Answer
The correct answer is: B. Fibromuscular dysplasia.
Figure 1 demonstrates findings consistent with renal fibromuscular dysplasia (FMD) including multifocal stenosis of the left renal artery and a saccular aneurysm.
FMD is a noninflammatory, nonatherosclerotic disease process which affects medium-sized arteries most commonly in middle aged women leading to vascular abnormalities such as arterial stenosis, occlusion, aneurysm and dissection.1 While the pathogenesis of FMD remains unclear, registry data shows that the renal and carotid arteries are the mostly commonly affected vascular beds.2 Patients often present with non-specific symptoms including headaches and pulsatile tinnitus; however, 67% of FMD patients present with new-onset hypertension, which is usually due to renovascular disease.2
Evaluation for renal FMD typically begins with a non-invasive imaging study such as renal artery duplex ultrasound, computed tomographic angiography or magnetic resonance angiography. Invasive catheter-based renal angiography remains the gold standard imaging modality for diagnosis of renal FMD.3 On angiography, renal FMD most commonly manifests as a multifocal stenosis with post-stenotic dilatations resulting in the classic "strings on a bead" pattern; however, aneurysms, dissections, unifocal stenoses and long tubular stenoses can also be seen.3 Contrary to atherosclerotic renal artery disease which usually affects the ostial and proximal vessel, renal FMD tends to occur in the mid to distal vessel.4 Notably, visual assessment of angiographic stenosis in renal FMD can be inaccurate, so invasive pressure gradient assessment is necessary to assess need for intervention.5
There is no randomized controlled trial data to guide renal artery intervention in patients with renal FMD, so the current management approach is based primarily on observational studies. Commonly accepted indications for renal artery intervention include new onset hypertension of short duration (with goal to cure hypertension), resistant hypertension, renal artery aneurysm, renal artery dissection, preservation of renal function and branch renal artery disease with hypertension.3 When anatomically feasible, percutaneous intervention is preferred over surgical intervention due to lower risk of adverse events with similar procedural success rates.3 While complex pathology such as renal aneurysm or dissection may require stent placement, most FMD can be successfully treated with percutaneous transluminal angioplasty (PTA) resulting in cure of hypertension in 40-50% of patients.3 Reassessment of pressure gradient is recommended after PTA to confirm improvement in stenosis as angiography may not necessarily show full resolution of the stenosis.5
In this case, the multifocal stenosis in the left renal artery was found to be significant on pressure gradient assessment, so the patient underwent PTA of the left renal artery. Figure 2 shows the post-intervention renal angiography result with improvement in stenosis. There was no pressure gradient across the lesion after PTA. The patient's hypertension was cured following PTA, and all anti-hypertensives were stopped within 1 month of her procedure. She was subsequently referred to vascular surgery and underwent successful stent graft placement for exclusion of the left renal artery aneurysm.
Figure 2: Post PTA Renal Angiogram
Figure 2
References
Olin JW, Froehlich J, Gu X, et al. The United States registry for fibromuscular dysplasia: results in the first 447 patients. Circulation 2012;125:3182-90.
Kim ESH, Olin JW, Froehlich JB, et al. Clinical manifestations of fibromuscular dysplasia vary by patient sex: a report of the United States registry for fibromuscular dysplasia. J Am Coll Cardiol 2013;62:2026-8.
Olin JW, Gornik HL, Bacharach JM, et al. Fibromuscular dysplasia: state of the science and critical unanswered questions: a scientific statement from the American Heart Association. Circulation 2014;129:1048-78.
Dworkin LD, Cooper CJ. Clinical practice. Renal-artery stenosis. N Engl J Med 2009;361:1972-8.
Prasad A, Zafar N, Mahmud E. Assessment of renal artery fibromuscular dysplasia: angiography, intravascular ultrasound (with virtual histology), and pressure wire measurements. Catheter Cardiovasc Interv 2009;74:260-4.