A 44-year-old woman with history of hypertension and nonischemic cardiomyopathy presents to the emergency department (ED) with palpitations consistent of a fluttering sensation in her chest, accompanied by dizziness, lightheadedness and fatigue.
Her echocardiogram shows normal LV size and systolic function with LVEF 55 - 60%.
Her exercise treadmill myocardial perfusion stress test is negative for inducible ischemia.
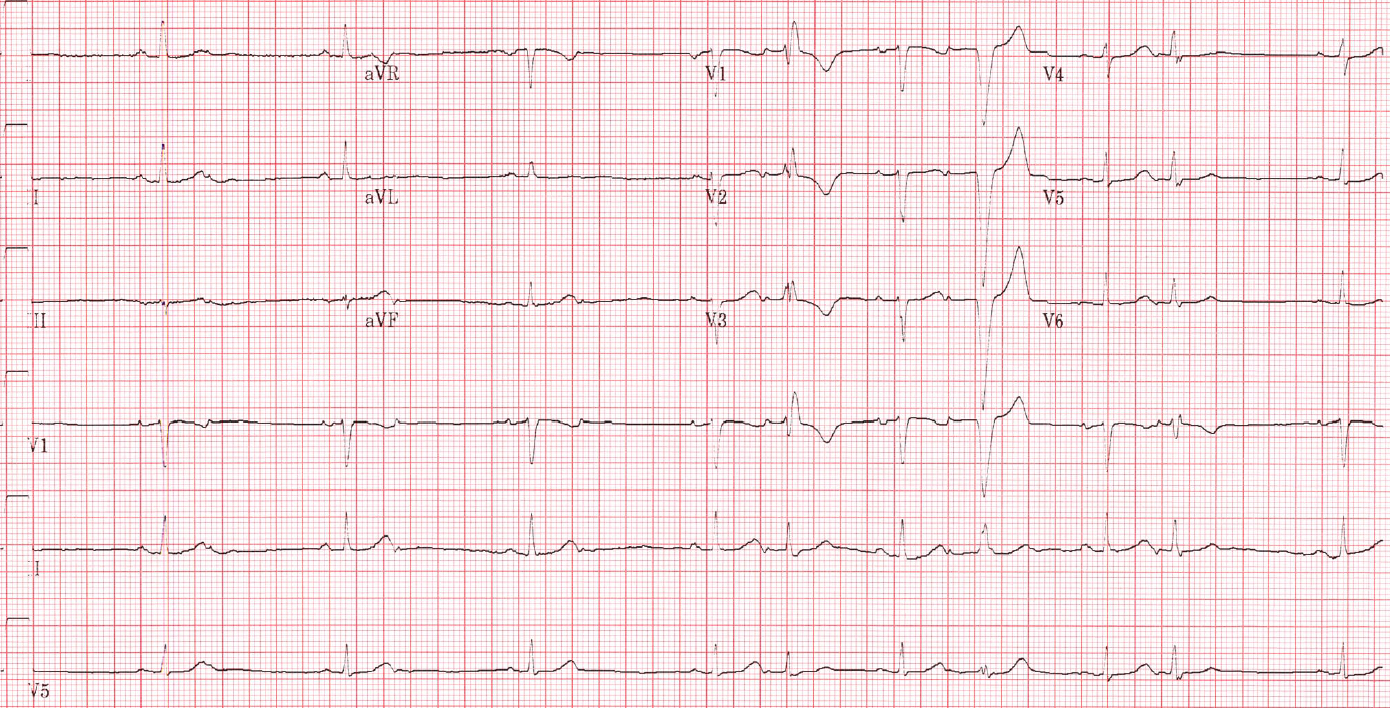
The following is her 12 lead electrocardiogram (ECG) during her clinic visit (Figure 1).
Figure 1
Figure 1
The ECG shows which of the following?
Show Answer
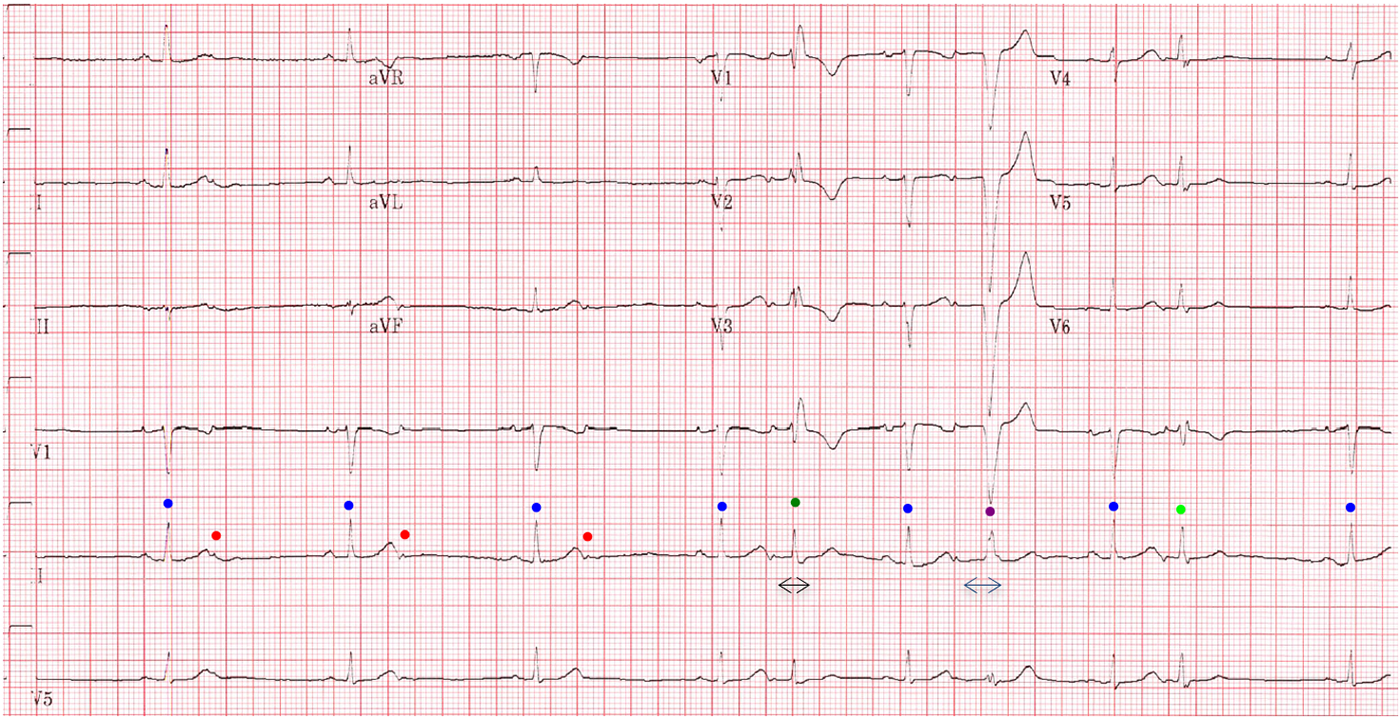
The correct answer is: C. Sinus rhythm with blocked premature atrial contraction (PACs) and PACs with aberrancy.
The blue dots in Figure 2 indicate sinus beats. The red dots are blocked premature atrial contractions that occur when the AV node is still in the absolute refractory period (ARP) and has not yet recovered. The P wave in the blocked PACs is different than during sinus rhythm; therefore, Answer choice A is incorrect as this is not second degree AV block.
PACs with aberrancy occurs when the PAC arrives to His-Purkinje system when one of its branches is in ARP or the relative refractory period (RRP).
The green dot represents PAC with right bundle branch block (RBBB) pattern, since the PAC conducts before the recovery of the right bundle from its ARP. The lime green dot represents a PAC with incomplete RBBB because the right bundle is in RRP and has partially recovered. This is eponymously known as Ashman's phenomenon, which happens as a sequence of a long-short cycle, leading to aberrancy in the premature beat.1
The purple dot is a PAC with left bundle branch block (LBBB), since the PAC conducts before the recovery of the left bundle from its ARP. Please note that the PR interval in the PAC with LBBB pattern is longer than the PR interval in the PAC with RBBB pattern as well as the sinus beat. This is due to delay in the AV node which will give enough time for the RBBB to recover and transition LBBB to ARP.
The RBBB pattern is commonly seen compared to a LBBB pattern because of the longer refractory period of the right bundle branch. This aberration is physiologic and does not require a permanent pacemaker. Suppression of the PACs may be accomplished by titration of a beta-blocker, and if the patient continues to be symptomatic, antiarrhythmic therapy may be considered. Catheter ablation is also an option, but reserved for cases which are refractory to pharmacologic therapy.
Options B and D are incorrect since wide QRS complexes are proceeded with P waves.
Figure 2
Figure 2
References
Gouaux JL, Ashman R. Auricular fibrillation with aberration simulating ventricular paroxysmal tachycardia. American Heart Journal 1947;34:366-73.