An 11-year-old previously healthy female child presented to the emergency department for 4 days of cough, congestion, and malaise that progressed to dyspnea, pallor, cyanosis, and weakness. Over the prior several months, she had experienced intermittent swelling of her hands and lower extremities, worsening night sweats and posterior uveitis for which an infectious work-up was negative. On initial exam, she was dyspneic with poor perfusion as evident by cool extremities and poor capillary refill. Chest x-ray showed significant cardiomegaly (Figure 1). Electrocardiogram (ECG) showed sinus tachycardia with right atrial enlargement and left ventricular (LV) hypertrophy (Figure 2). Initial echocardiogram showed an ejection fraction of 10% without pericardial effusion, and her B-type natriuretic peptide was >5000 ng/L. She had an acute event consisting of a seizure and asystolic cardiac arrest and underwent 48 minutes of cardiopulmonary resuscitation. She underwent the hypothermia protocol for 48 hours and was transitioned to venoarterial (VA) extracorporeal membrane oxygenation (ECMO) for intractable low cardiac output and acidosis. She remained on VA ECMO for 4 days. After ECMO decannulation, her echocardiogram showed a moderately dilated LV with an ejection fraction of 15% and moderate to severe diastolic dysfunction (Figure 3) while on a milrinone drip of 0.75 mcg/kg/min. Cardiac transplantation work-up was initiated. While in the pediatric intensive care unit, she was noted to have systolic blood pressures up to 150 mmHg and diastolic blood pressures up to 96 mmHg despite several doses of intravenous hydralazine, and her heart rate was persistently 130-140 beats per minute. Magnetic resonance imaging of the brain showed evidence of several acute emboli without significant mass effect, midline shift, or hydrocephalus. Family history was notable for a mother with rheumatoid arthritis and maternal grandmother with hyperthyroidism. Her antinuclear antibody test was normal.
Figure 1: Chest X-Ray Shows Cardiomegaly
Figure 1
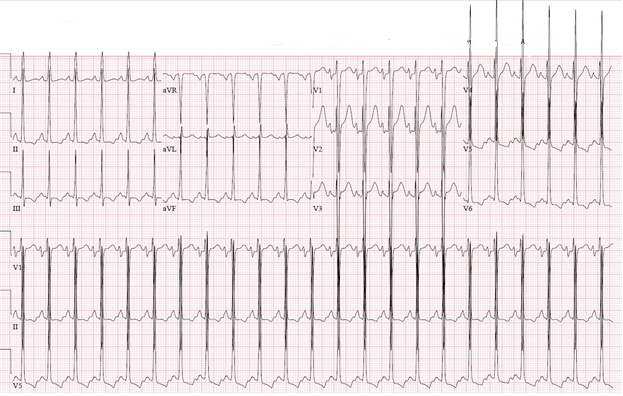
Figure 2: Twelve-Lead ECG Shows LV Hypertrophy With Strain Pattern and Right Atrial Enlargement
Figure 2
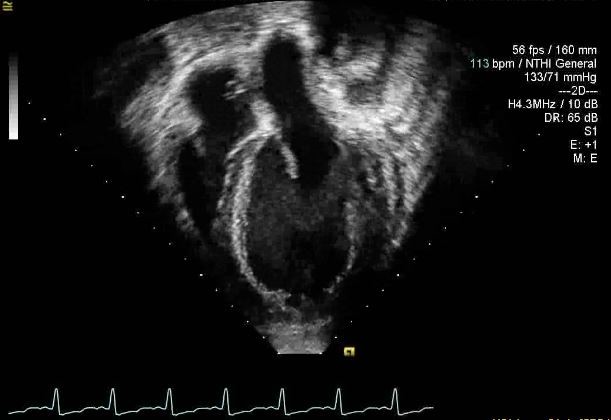
Figure 3: Apical 4-Chamber View Shows a Dilated and Hypertrophied LV
Figure 3
Her LV end diastolic dimension was 6.2 cm (Z-score = 3.94).
Her LV end diastolic dimension was 6.2 cm (Z-score = 3.94).
Which test is most likely to diagnose the cause of this patient's heart failure?
Show Answer
The correct answer is: C. Urine metanephrines
Our patient's initial presentation and imaging were suspicious for either infectious myocarditis or an underlying genetic cardiomyopathy. Typically with these etiologies, however, patients who present in cardiogenic shock have hypoperfusion and hypotension. Likewise, thyrotoxicosis-induced cardiomyopathy secondary to Grave's disease would present with hypotension.1 Her thyroid-stimulating hormone and free thyroxine were both normal. Cardiac involvement in children with systemic lupus is most commonly pericarditis.2 A normal antinuclear antibody, lack of effusion, and no characteristic ECG findings make this diagnosis unlikely. Although long-term patients with lupus are at risk for heart failure,3 acute fulminant myocarditis associated with lupus is rare and would also present with cardiogenic shock and hypotension. Instead, our patient was significantly hypertensive with an ejection fraction of 15%, requiring several doses of intravenous medication to control blood pressure. As a result, a more thorough work-up for hypertension was completed. A renal ultrasound showed a large heterogeneous left suprarenal mass suggestive of pheochromocytoma or adenocarcinoma (Figure 4). In the setting of hypertension, urine-free metanephrine was ordered and was 18 nmol/L (normally less than 0.9 nmol/L), supporting the diagnosis of pheochromocytoma. A PGLNext panel through Ambry Genetics (Aliso Viejo, CA) involving sequencing and deletion/duplication analysis of 12 genes associated with hereditary paraganglioma-pheochromocytoma was completed and was negative for any clinically significant changes. Ophthalmologic evaluation while inpatient showed neuroretinitis with optic nerve edema and macular swelling with exudates, which was thought to be secondary to recurrent episodes of hypertension. Our patient was successfully bridged to surgical therapy with the use of extra-corporeal life support. Pre-operatively, her blood pressure was controlled using prazosin. Esmolol was at the bedside in case of severe rebound hypertension, but it was not needed. She was, however, maintained on her milrinone drip and eventually started on low-dose carvedilol. With treatment of her pheochromocytoma and normalization of her blood pressure, her macular edema, disc edema, and exudates improved.
Figure 4: Renal Ultrasound Shows a Suprarenal Mass Measuring 6.91 x 5.63 cm
Figure 4
Pheochromocytoma is a rare catecholamine-producing neuroendocrine tumor that occurs most commonly in adults but occurs in children about 10% of the time. The classic presentation consists of hypertension, headache, sweating, and tremor.4 Although uncommon, severe cardiomyopathy and cardiogenic shock may occur and require the use of mechanical circulatory support.5,6 The mechanism of catecholamine-induced cardiomyopathy is debated but likely involves a combination of coronary artery spasm, cellular toxicity, or myocardial stunning.7,8 Once the malignancy is surgically removed, function often returns to normal.9,10 Similarly, our patient's LV ejection fraction was 56% 7 months post left adrenalectomy, and we have begun weaning her heart failure medications.
In conclusion, pheochromocytoma should be included on the differential for acute cardiogenic shock in pediatric patients, especially if unexplained hypertension is present.
References
Ertek S, Cicero AF. Hyperthyroidism and cardiovascular complications: a narrative review on the basis of pathophysiology. Arch Med Sci 2013;9:944-52.
Weiss JE. Pediatric systemic lupus erythematosus: more than a positive antinuclear antibody. Pediatr Rev 2012;33:62-73.
Kim CH, Al-Kindi SG, Jandali B, Askari AD, Zacharias M, Oliveira GH. Incidence and risk of heart failure in systemic lupus erythematosus. Heart 2017;103:227-33.
Bholah R, Bunchman TE. Review of Pediatric Pheochromocytoma and Paraganglioma. Front Pediatr 2017;5:155.
Hekimian G, Kharcha F, Bréchot N, et al. Extracorporeal membrane oxygenation for pheochromocytoma-induced cardiogenic shock. Ann Intensive Care 2016;6:117.
Sojod G, Diana M, Wall J, D'Agostino J, Mutter D, Marescaux J. Successful extracorporeal membrane oxygenation treatment for pheochromocytoma-induced acute cardiac failure. Am J Emerg Med 2012;30:1017.e1-3.
Iio K, Sakurai S, Kato T, et al. Endomyocardial biopsy in a patient with hemorrhagic pheochromocytoma presenting as inverted Takotsubo cardiomyopathy. Heart Vessels 2013;28:255-63.
Kodama T, Agozzino M, Pellegrini C, et al. Endomyocardial Biopsy in acute cardiogenic shock: Diagnosis of pheochromocytoma. Int J Cardiol 2016;202:897-9.
Bausch B, Wellner U, Bausch D, et al. Long-term prognosis of patients with pediatric pheochromocytoma. Endocr Relat Cancer 2013;21:17-25.
Flam B, Broomé M, Frenckner B, Bränström R, Bell M. Pheochromocytoma-Induced Inverted Takotsubo-Like Cardiomyopathy Leading to Cardiogenic Shock Successfully Treated With Extracorporeal Membrane Oxygenation. J Intensive Care Med 2015;30:365-72.